ICES, Toronto, Ontario, Canada.
Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, Canada.
PLoS One. 2021 Jan 7;16(1):e0244746. doi: 10.1371/journal.pone.0244746. eCollection 2021.
Routinely collected health administrative data can be used to efficiently assess disease burden in large populations, but it is important to evaluate the validity of these data. The objective of this study was to develop and validate International Classification of Disease 10th revision (ICD -10) algorithms that identify laboratory-confirmed influenza or laboratory-confirmed respiratory syncytial virus (RSV) hospitalizations using population-based health administrative data from Ontario, Canada.
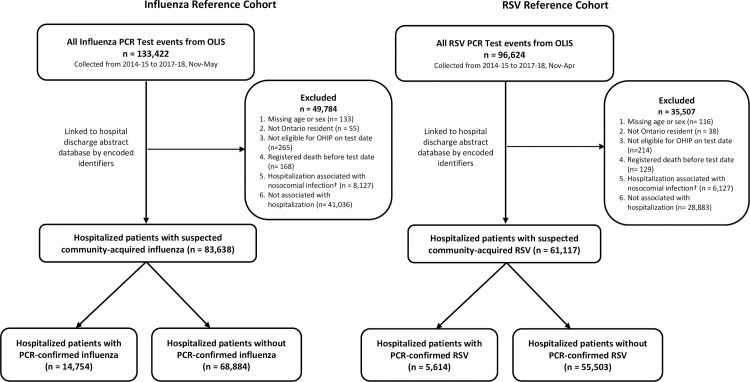
Influenza and RSV laboratory data from the 2014-15, 2015-16, 2016-17 and 2017-18 respiratory virus seasons were obtained from the Ontario Laboratories Information System (OLIS) and were linked to hospital discharge abstract data to generate influenza and RSV reference cohorts. These reference cohorts were used to assess the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the ICD-10 algorithms. To minimize misclassification in future studies, we prioritized specificity and PPV in selecting top-performing algorithms.
83,638 and 61,117 hospitalized patients were included in the influenza and RSV reference cohorts, respectively. The best influenza algorithm had a sensitivity of 73% (95% CI 72% to 74%), specificity of 99% (95% CI 99% to 99%), PPV of 94% (95% CI 94% to 95%), and NPV of 94% (95% CI 94% to 95%). The best RSV algorithm had a sensitivity of 69% (95% CI 68% to 70%), specificity of 99% (95% CI 99% to 99%), PPV of 91% (95% CI 90% to 91%) and NPV of 97% (95% CI 97% to 97%).
We identified two highly specific algorithms that best ascertain patients hospitalized with influenza or RSV. These algorithms may be applied to hospitalized patients if data on laboratory tests are not available, and will thereby improve the power of future epidemiologic studies of influenza, RSV, and potentially other severe acute respiratory infections.
通过使用基于人群的健康管理数据,可有效地评估大人群的疾病负担,而常规收集的健康管理数据可以做到这一点,但重要的是要评估这些数据的有效性。本研究的目的是开发和验证使用加拿大安大略省人群健康管理数据识别实验室确诊流感或实验室确诊呼吸道合胞病毒(RSV)住院的国际疾病分类第 10 版(ICD-10)算法。
从安大略省实验室信息系统(OLIS)获得了 2014-15、2015-16、2016-17 和 2017-18 呼吸道病毒季节的流感和 RSV 实验室数据,并将其与医院出院摘要数据进行了链接,以生成流感和 RSV 参考队列。使用这些参考队列来评估 ICD-10 算法的灵敏度、特异性、阳性预测值(PPV)和阴性预测值(NPV)。为了在未来的研究中尽量减少错误分类,我们在选择表现最佳的算法时优先考虑特异性和 PPV。
分别纳入了 83638 例和 61117 例流感和 RSV 住院患者的参考队列。最佳流感算法的灵敏度为 73%(95%CI 72%至 74%),特异性为 99%(95%CI 99%至 99%),PPV 为 94%(95%CI 94%至 95%),NPV 为 94%(95%CI 94%至 95%)。最佳 RSV 算法的灵敏度为 69%(95%CI 68%至 70%),特异性为 99%(95%CI 99%至 99%),PPV 为 91%(95%CI 90%至 91%),NPV 为 97%(95%CI 97%至 97%)。
我们确定了两个最能确定因流感或 RSV 住院的患者的高特异性算法。如果无法获得实验室检测数据,这些算法可应用于住院患者,从而提高未来流感、RSV 以及潜在其他严重急性呼吸道感染的流行病学研究的效力。