Division of Endocrinology, Diabetes & Metabolism, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland.
JAMA Netw Open. 2021 Jan 4;4(1):e2030913. doi: 10.1001/jamanetworkopen.2020.30913.
Accurate clinical decision support tools are needed to identify patients at risk for iatrogenic hypoglycemia, a potentially serious adverse event, throughout hospitalization.
To predict the risk of iatrogenic hypoglycemia within 24 hours after each blood glucose (BG) measurement during hospitalization using a machine learning model.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study, conducted at 5 hospitals within the Johns Hopkins Health System, included 54 978 admissions of 35 147 inpatients who had at least 4 BG measurements and received at least 1 U of insulin during hospitalization between December 1, 2014, and July 31, 2018. Data from the largest hospital were split into a 70% training set and 30% test set. A stochastic gradient boosting machine learning model was developed using the training set and validated on internal and external validation.
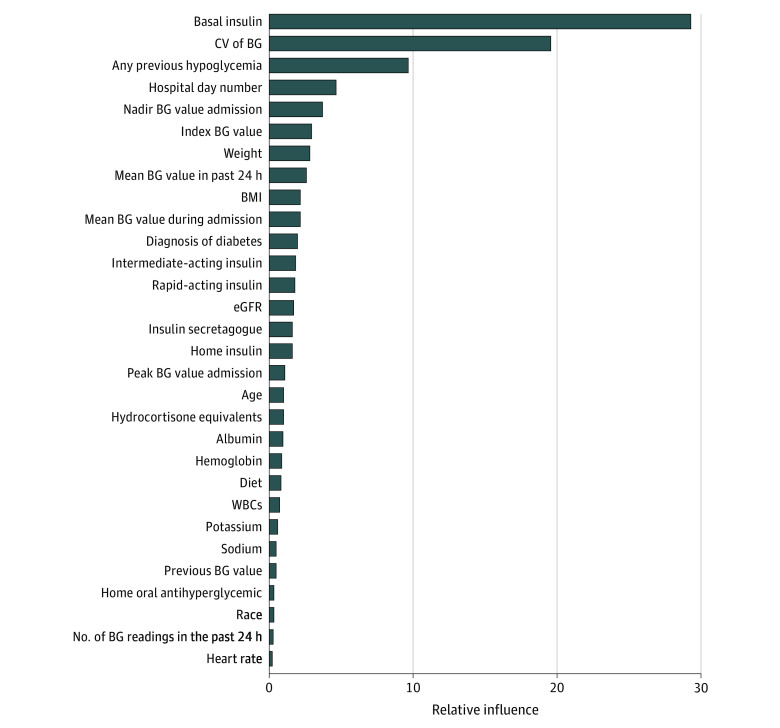
A total of 43 clinical predictors of iatrogenic hypoglycemia were extracted from the electronic medical record, including demographic characteristics, diagnoses, procedures, laboratory data, medications, orders, anthropomorphometric data, and vital signs.
Iatrogenic hypoglycemia was defined as a BG measurement less than or equal to 70 mg/dL occurring within the pharmacologic duration of action of administered insulin, sulfonylurea, or meglitinide.
This cohort study included 54 978 admissions (35 147 inpatients; median [interquartile range] age, 66.0 [56.0-75.0] years; 27 781 [50.5%] male; 30 429 [55.3%] White) from 5 hospitals. Of 1 612 425 index BG measurements, 50 354 (3.1%) were followed by iatrogenic hypoglycemia in the subsequent 24 hours. On internal validation, the model achieved a C statistic of 0.90 (95% CI, 0.89-0.90), a positive predictive value of 0.09 (95% CI, 0.08-0.09), a positive likelihood ratio of 4.67 (95% CI, 4.59-4.74), a negative predictive value of 1.00 (95% CI, 1.00-1.00), and a negative likelihood ratio of 0.22 (95% CI, 0.21-0.23). On external validation, the model achieved C statistics ranging from 0.86 to 0.88, positive predictive values ranging from 0.12 to 0.13, negative predictive values of 0.99, positive likelihood ratios ranging from 3.09 to 3.89, and negative likelihood ratios ranging from 0.23 to 0.25. Basal insulin dose, coefficient of variation of BG, and previous hypoglycemic episodes were the strongest predictors.
These findings suggest that iatrogenic hypoglycemia can be predicted in a short-term prediction horizon after each BG measurement during hospitalization. Further studies are needed to translate this model into a real-time informatics alert and evaluate its effectiveness in reducing the incidence of inpatient iatrogenic hypoglycemia.
需要准确的临床决策支持工具来识别住院期间发生潜在严重不良事件的医源性低血糖风险。
使用机器学习模型预测住院期间每次血糖 (BG) 测量后 24 小时内发生医源性低血糖的风险。
设计、设置和参与者:这项回顾性队列研究在约翰霍普金斯卫生系统的 5 家医院进行,包括 54978 例住院患者的 35147 例住院患者,这些患者在 2014 年 12 月 1 日至 2018 年 7 月 31 日期间至少有 4 次 BG 测量,并且在住院期间至少接受过 1 U 胰岛素治疗。最大医院的数据分为 70%的训练集和 30%的测试集。使用训练集开发了一个随机梯度提升机器学习模型,并在内部和外部验证中进行了验证。
从电子病历中提取了 43 个医源性低血糖的临床预测因素,包括人口统计学特征、诊断、手术、实验室数据、药物、医嘱、人体测量数据和生命体征。
医源性低血糖被定义为在给予的胰岛素、磺酰脲或米格列汀的药理作用持续时间内,BG 测量值低于或等于 70mg/dL。
这项队列研究包括 54978 例住院患者(35147 例住院患者;中位数[四分位数范围]年龄为 66.0[56.0-75.0]岁;27781 例[50.5%]男性;30429 例[55.3%]白人)来自 5 家医院。在 1612425 次指数 BG 测量中,50354 次(3.1%)随后在随后的 24 小时内发生医源性低血糖。在内部验证中,该模型的 C 统计量为 0.90(95%CI,0.89-0.90),阳性预测值为 0.09(95%CI,0.08-0.09),阳性似然比为 4.67(95%CI,4.59-4.74),阴性预测值为 1.00(95%CI,1.00-1.00),阴性似然比为 0.22(95%CI,0.21-0.23)。在外部验证中,该模型的 C 统计量范围为 0.86 至 0.88,阳性预测值范围为 0.12 至 0.13,阴性预测值为 0.99,阳性似然比范围为 3.09 至 3.89,阴性似然比范围为 0.23 至 0.25。基础胰岛素剂量、BG 变异系数和以前的低血糖发作是最强的预测因素。
这些发现表明,可以在住院期间每次 BG 测量后的短期预测期内预测医源性低血糖。需要进一步的研究将该模型转化为实时信息学警报,并评估其在降低住院患者医源性低血糖发生率方面的有效性。