Williams Kerry-Lynn, Renouf Tia S, Dubrowski Adam
Family Medicine, Memorial University of Newfoundland, Happy Valley-Goose Bay, CAN.
Emergency Medicine, Memorial University of Newfoundland, St. John's, CAN.
Cureus. 2020 Dec 8;12(12):e11965. doi: 10.7759/cureus.11965.
The emergency department is a complex practice environment into which numerous factors may introduce both human and system error. Emergency physicians have to assemble and manage multidisciplinary teams with a moment's notice to manage critically ill patients. The EM training programs across Canada are diverse with considerable variation among programs. Acquisition of both high acuity low occurrence (HALO) and crisis resource management (CRM) skills are crucial to the development of proficient emergency room physicians. Physicians and allied health workers were surveyed to identify potential causes of error in local emergency departments and to find simulation-driven solutions.
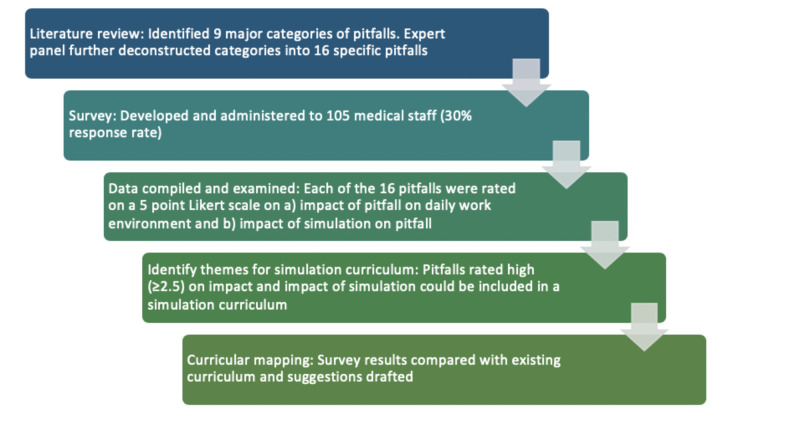
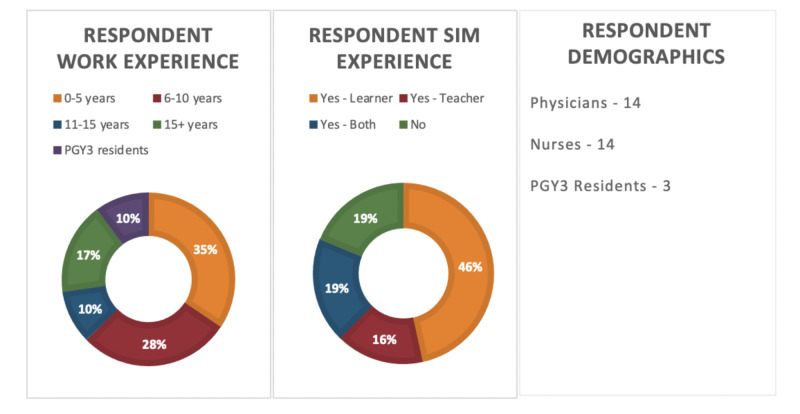
An anonymous survey was prepared to evaluate potential pitfalls of emergency care in St. John's, NL, Canada. It was distributed electronically to 108 medical staff, including physicians, nurses, and postgraduate year three (PGY3) residents. Respondents were asked about their experience with simulation education, and whether or not they feel that there is an opportunity for it in postgraduate emergency medicine training.
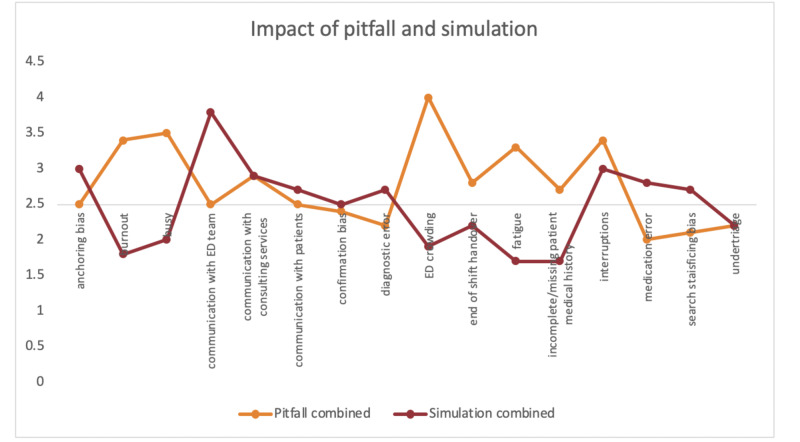
The response rate was 30%. Communication - with the emergency department team, consulting services, and patients - was identified as a potential topic for simulation, along with interruptions. Burnout, busy department, departmental crowding, end of shift handover, and incomplete/missing patient medical history were identified as topics that should be included in the emergency medicine curriculum. Following a review with the simulation expert panel, it was determined that end of shift handover could also be incorporated as a simulation in the existing curriculum.
This survey looked at pitfalls in emergency medicine through a CRM lens. Six pitfalls were identified as important for patient safety, but not best addressed with simulation. These could be incorporated into the half-day curriculum as didactic lectures. Four important patient safety pitfalls were identified that could potentially be addressed with simulation and incorporated in the existing emergency medicine simulation curriculum.
急诊科是一个复杂的执业环境,众多因素可能导致人为和系统错误。急诊医生必须在接到通知后立即组建并管理多学科团队,以救治重症患者。加拿大各地的急诊医学培训项目各不相同,项目之间存在很大差异。掌握高敏锐度低发生率(HALO)技能和危机资源管理(CRM)技能对于培养熟练的急诊室医生至关重要。对医生和专职医护人员进行了调查,以确定当地急诊科潜在的错误原因,并寻找模拟驱动的解决方案。
准备了一项匿名调查,以评估加拿大纽芬兰与拉布拉多省圣约翰市急诊护理的潜在隐患。该调查以电子方式分发给108名医务人员,包括医生、护士和三年级住院医师(PGY3)。受访者被问及他们的模拟教育经历,以及他们是否认为在研究生急诊医学培训中有开展模拟教育的机会。
回复率为30%。与急诊科团队、咨询服务部门和患者的沟通以及干扰因素被确定为模拟的潜在主题。职业倦怠、科室繁忙、科室拥挤、交接班和患者病史不完整/缺失被确定为急诊医学课程应涵盖的主题。在与模拟专家小组进行审查后,确定交接班也可纳入现有课程的模拟内容。
本次调查从CRM的角度审视了急诊医学中的隐患。确定了六个对患者安全很重要但无法通过模拟得到最佳解决的隐患。这些隐患可以作为理论讲座纳入半天的课程中。确定了四个重要的患者安全隐患,这些隐患有可能通过模拟来解决,并纳入现有的急诊医学模拟课程中。