Coury Jennifer, Miech Edward J, Styer Patricia, Petrik Amanda F, Coates Kelly E, Green Beverly B, Baldwin Laura-Mae, Shapiro Jean A, Coronado Gloria D
Oregon Rural Practice-based Research Network, Oregon Health & Science University, 3181 S.W. Sam Jackson Park Rd., Mail Code L222, Portland, OR, 97239, USA.
Center for Health Services Research, Regenstrief Institute, Indianapolis, IN, USA.
Implement Sci Commun. 2021 Jan 11;2(1):5. doi: 10.1186/s43058-020-00104-7.
Mailed fecal immunochemical testing (FIT) programs can improve colorectal cancer (CRC) screening rates, but health systems vary how they implement (i.e., adapt) these programs for their organizations. A health insurance plan implemented a mailed FIT program (named BeneFIT), and participating health systems could adapt the program. This multi-method study explored which program adaptations might have resulted in higher screening rates.
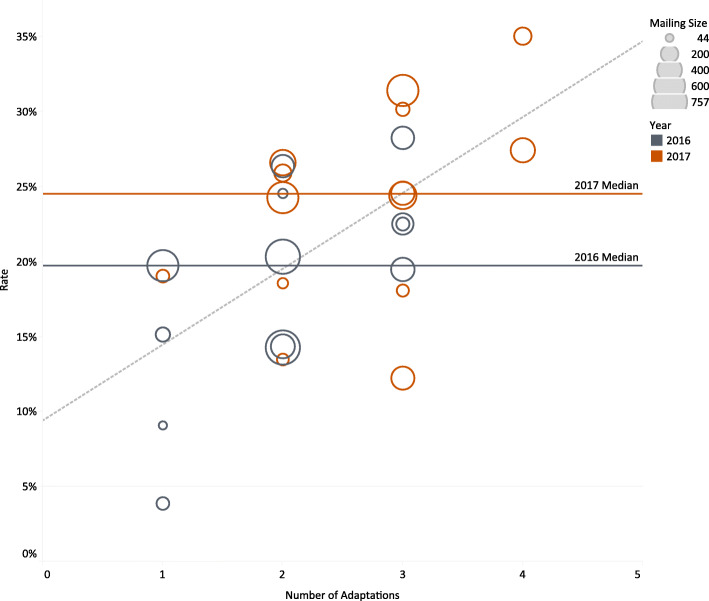
First, we conducted a descriptive analysis of CRC screening rates by key health system characteristics and program adaptations. Second, we generated an overall model by fitting a weighted regression line to our data. Third, we applied Configurational Comparative Methods (CCMs) to determine how combinations of conditions were linked to higher screening rates. The main outcome measure was CRC screening rates.
Seventeen health systems took part in at least 1 year of BeneFIT. The overall screening completion rate was 20% (4-28%) in year 1 and 25% (12-35%) in year 2 of the program. Health systems that used two or more adaptations had higher screening rates, and no single adaptation clearly led to higher screening rates. In year 1, small systems, with just one clinic, that used phone reminders (n = 2) met the implementation success threshold (≥ 19% screening rate) while systems with > 1 clinic were successful when offering a patient incentive (n = 4), scrubbing mailing lists (n = 4), or allowing mailed FIT returns with no other adaptations (n = 1). In year 2, larger systems with 2-4 clinics were successful with a phone reminder (n = 4) or a patient incentive (n = 3). Of the 10 systems that implemented BeneFIT in both years, seven improved their CRC screening rates in year 2.
Health systems can choose among many adaptations and successfully implement a health plan's mailed FIT program. Different combinations of adaptations led to success with health system size emerging as an important contextual factor.
邮寄粪便免疫化学检测(FIT)项目可提高结直肠癌(CRC)筛查率,但各卫生系统在将这些项目应用于其组织时(即进行调整)方式各异。一项医疗保险计划实施了一项邮寄FIT项目(名为BeneFIT),参与的卫生系统可对该项目进行调整。这项多方法研究探讨了哪些项目调整可能导致更高的筛查率。
首先,我们按关键卫生系统特征和项目调整对CRC筛查率进行了描述性分析。其次,通过对数据拟合加权回归线生成了一个总体模型。第三,我们应用组态比较法(CCMs)来确定条件组合与更高筛查率之间的关联。主要结局指标为CRC筛查率。
17个卫生系统参与了至少一年的BeneFIT项目。该项目第一年的总体筛查完成率为20%(4%-28%),第二年为25%(12%-35%)。采用两种或更多种调整措施的卫生系统筛查率更高,且没有单一的调整措施能明显提高筛查率。在第一年,仅有一家诊所的小型系统在使用电话提醒时(n = 2)达到了实施成功阈值(筛查率≥19%),而拥有多家诊所的系统在提供患者激励措施(n = 4)、清理邮件列表(n = 4)或允许邮寄FIT检测结果而无其他调整措施时(n = 1)取得了成功。在第二年,拥有2至4家诊所的较大型系统在采用电话提醒(n = 4)或患者激励措施(n = 3)时取得了成功。在两年均实施BeneFIT项目的10个系统中,有7个系统在第二年提高了CRC筛查率。
卫生系统可在多种调整措施中进行选择,并成功实施健康计划的邮寄FIT项目。不同的调整组合取得了成功,卫生系统规模成为一个重要的背景因素。