Jenkins David A, Martin Glen P, Sperrin Matthew, Riley Richard D, Debray Thomas P A, Collins Gary S, Peek Niels
Division of Informatics, Imaging and Data Science, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK.
NIHR Greater Manchester Patient Safety Translational Research Centre, The University of Manchester, Manchester, UK.
Diagn Progn Res. 2021 Jan 11;5(1):1. doi: 10.1186/s41512-020-00090-3.
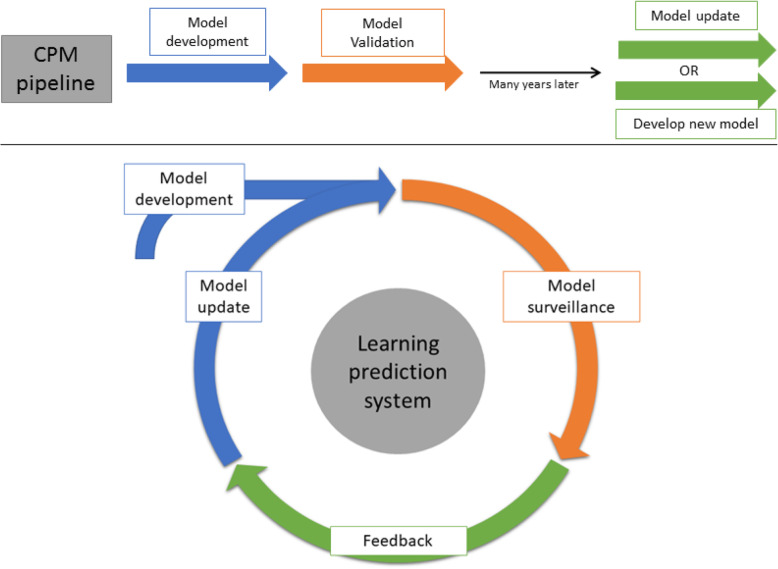
Clinical prediction models (CPMs) have become fundamental for risk stratification across healthcare. The CPM pipeline (development, validation, deployment, and impact assessment) is commonly viewed as a one-time activity, with model updating rarely considered and done in a somewhat ad hoc manner. This fails to address the fact that the performance of a CPM worsens over time as natural changes in populations and care pathways occur. CPMs need constant surveillance to maintain adequate predictive performance. Rather than reactively updating a developed CPM once evidence of deteriorated performance accumulates, it is possible to proactively adapt CPMs whenever new data becomes available. Approaches for validation then need to be changed accordingly, making validation a continuous rather than a discrete effort. As such, "living" (dynamic) CPMs represent a paradigm shift, where the analytical methods dynamically generate updated versions of a model through time; one then needs to validate the system rather than each subsequent model revision.
临床预测模型(CPMs)已成为医疗保健领域风险分层的基础。CPM流程(开发、验证、部署和影响评估)通常被视为一次性活动,很少考虑模型更新,且更新方式有些随意。这未能解决随着人群和护理路径的自然变化,CPM的性能会随时间恶化这一事实。CPMs需要持续监测以维持足够的预测性能。与其在性能恶化的证据积累后被动更新已开发的CPM,不如在有新数据可用时主动调整CPMs。相应地,验证方法也需要改变,使验证成为一项持续而非离散的工作。因此,“动态”(实时)CPMs代表了一种范式转变,即分析方法随时间动态生成模型的更新版本;然后需要验证系统,而不是验证每个后续的模型修订版。