Yamada Yosuke, Harada Makoto, Hara Yuuta, Iwabuchi Ryohei, Hashimoto Koji, Yamamoto Shuhei, Kamijo Yuji
Department of Nephrology, Shinshu University School of Medicine, 3-1-1 Asahi, Matsumoto, Nagano, 390-8621, Japan.
Department of Rehabilitation, Shinshu University Hospital, 3-1-1 Asahi, Matsumoto, Nagano, 390-8621, Japan.
Arthritis Res Ther. 2021 Jan 14;23(1):28. doi: 10.1186/s13075-021-02415-z.
To assess through systematic review and meta-analysis whether plasma exchange (PE) is associated with prognosis in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) patients.
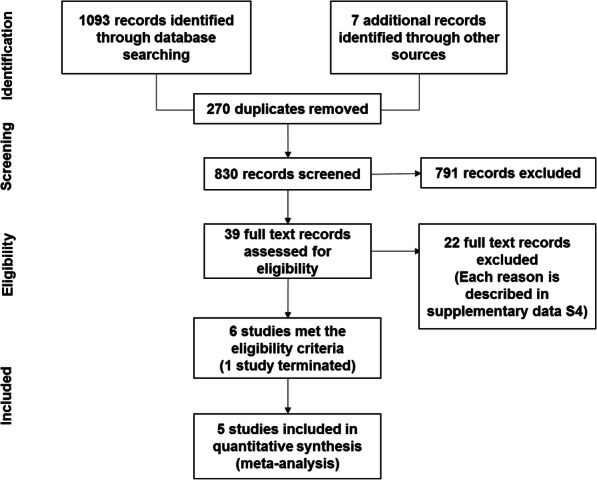
A systematic search of PubMed, MEDLINE, Embase, and CENTRAL databases from inception to 17 June 2020 was conducted. Ongoing or unpublished trials were also searched in ClinicalTrials.gov and the World Health Organization trials portal. Randomised controlled trials (RCTs) comparing PE vs. non-PE in AAV patients (microscopic polyangiitis [MPA], granulomatosis with polyangiitis [GPA], or eosinophilic granulomatosis with polyangiitis [EGPA]) were included. The combined risk ratio (RR) was calculated by the random-effects model using the Mantel-Haenszel method. Heterogeneity was measured using the I statistic. Primary outcomes were mortality, clinical remission (CR), and adverse events (AEs).
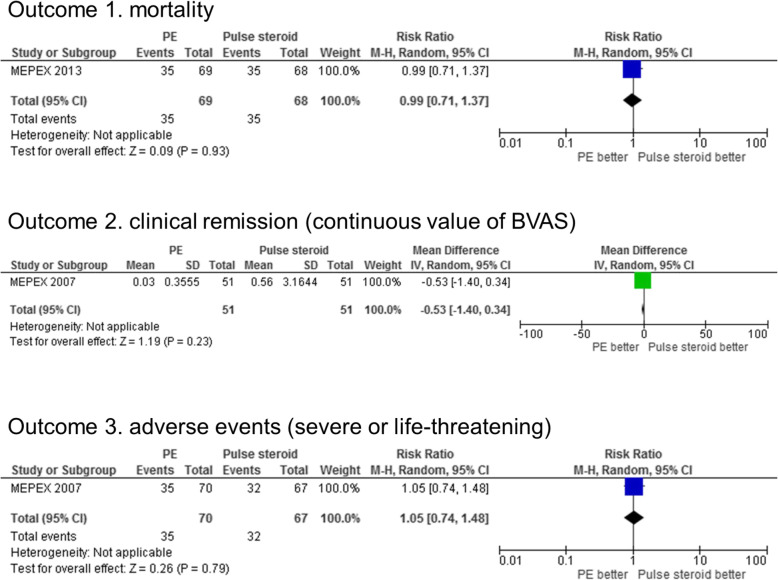
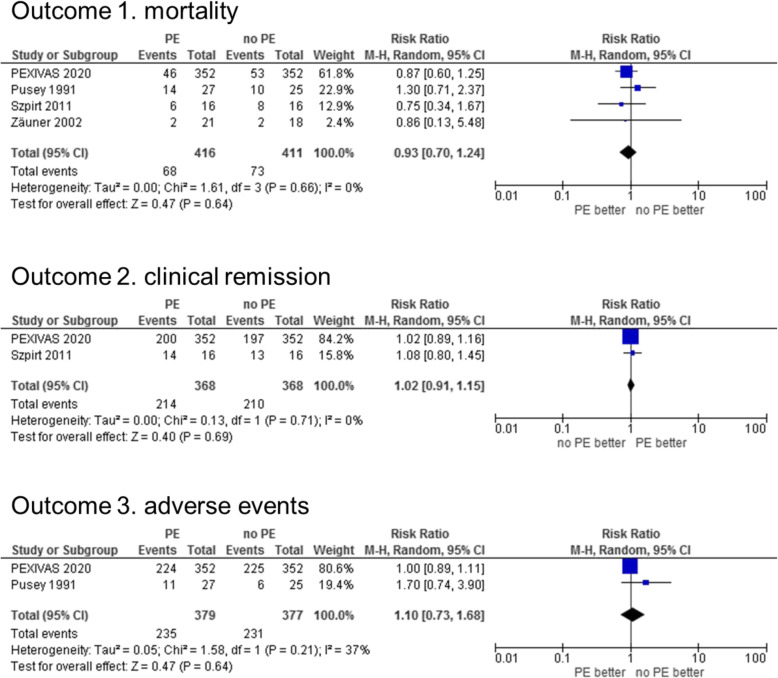
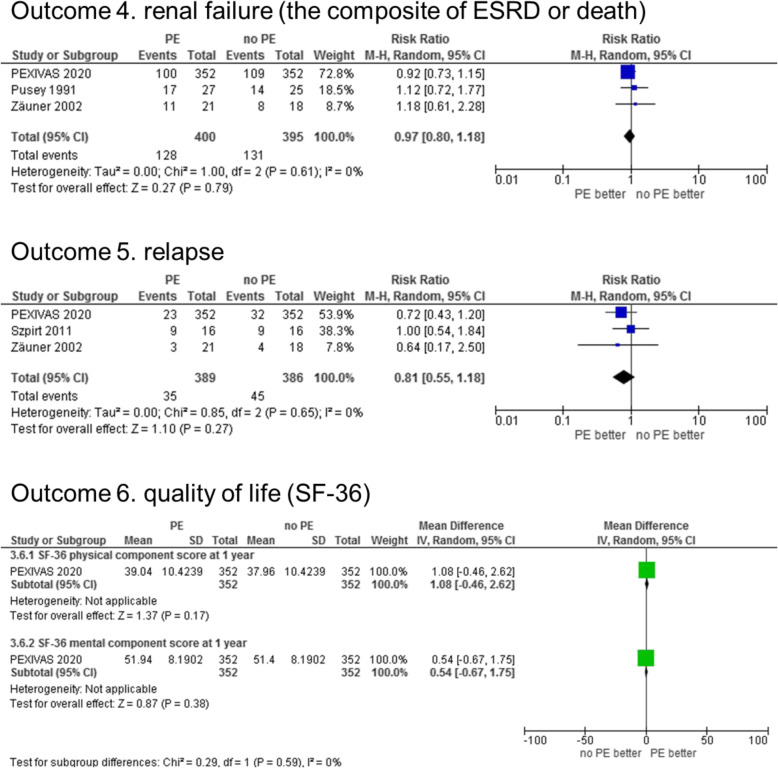
Four RCTs comparing PE vs. no PE (N = 827) and 1 RCT comparing PE vs. pulse steroid treatment (N = 137) were included. All participants were MPA or GPA patients (no EGPA patients). PE was not associated with main primary outcomes compared with no PE (mortality RR 0.93 [95% confidence interval {CI} 0.70-1.24], I = 0%; CR RR 1.02 [95% CI 0.91-1.15], I = 0%; and AE RR 1.10 [95% CI 0.73-1.68], I = 37%) or pulse steroid (mortality RR 0.99 [95% CI 0.71-1.37]; CR [the Birmingham Vasculitis Activity score] mean difference - 0.53 [95% CI - 1.40-0.34]; and AE RR 1.05 [95% CI 0.74-1.48]). Focusing on the early treatment phases, PE was associated with a reduction in end-stage renal disease incidence compared with both no PE (PE 1/43 vs. no PE 10/41; RR 0.14 [0.03-0.77] at 3 months) and pulse steroid (PE 11/70 vs. pulse steroid 23/67; RR 0.46 [0.24-0.86] at 3 months).
We carried out a systematic review and meta-analysis targeting all AAV patients, including MPA, GPA, and EGPA. In AAV patients, performing PE was not associated with the risk of mortality, CR, and AE. No RCT exists evaluating the efficacy of PE for EGPA; hence, this is required in the future. The results may affect the development of guidelines for AAV and may indicate the direction of future clinical research on AAV.
UMIN R000045239 , PROSPERO CRD42020182566 .
通过系统评价和荟萃分析评估血浆置换(PE)是否与抗中性粒细胞胞浆抗体(ANCA)相关血管炎(AAV)患者的预后相关。
对PubMed、MEDLINE、Embase和CENTRAL数据库从创建至2020年6月17日进行系统检索。还在ClinicalTrials.gov和世界卫生组织试验门户网站中检索了正在进行或未发表的试验。纳入比较AAV患者(显微镜下多血管炎[MPA]、肉芽肿性多血管炎[GPA]或嗜酸性肉芽肿性多血管炎[EGPA])接受PE与未接受PE的随机对照试验(RCT)。采用Mantel-Haenszel方法通过随机效应模型计算合并风险比(RR)。使用I²统计量测量异质性。主要结局为死亡率、临床缓解(CR)和不良事件(AE)。
纳入了4项比较PE与未接受PE(N = 827)以及1项比较PE与脉冲类固醇治疗(N = 137)的RCT。所有参与者均为MPA或GPA患者(无EGPA患者)。与未接受PE相比,PE与主要主要结局无关(死亡率RR 0.93[95%置信区间{CI}0.70 - 1.24],I² = 0%;CR RR 1.02[95%CI 0.91 - 1.15],I² = 0%;AE RR 1.10[95%CI 0.73 - 1.68],I² = 37%)或脉冲类固醇(死亡率RR 0.99[95%CI 0.71 - 1.37];CR[伯明翰血管炎活动评分]平均差−0.53[95%CI - 1.40 - 0.34];AE RR 1.05[95%CI 0.74 - 1.48])。聚焦于早期治疗阶段,与未接受PE(3个月时PE 1/43 vs.未接受PE 10/41;RR 0.14[0.03 - 0.77])和脉冲类固醇(3个月时PE 11/70 vs.脉冲类固醇23/67;RR 0.46[0.24 - 0.86])相比,PE与终末期肾病发病率降低相关。
我们针对所有AAV患者,包括MPA、GPA和EGPA进行了系统评价和荟萃分析。在AAV患者中,进行PE与死亡率、CR和AE风险无关。不存在评估PE对EGPA疗效的RCT;因此,未来需要进行此类研究。这些结果可能会影响AAV指南的制定,并可能为AAV未来的临床研究指明方向。
UMIN R000045239,PROSPERO CRD4202××××××(原文此处PROSPERO编号不全,推测可能是录入错误,正常应完整呈现) 。