Jain Dhruv, Mohan Virender K, Bhoi Debesh, Batra Ravinder K, Kashyap Lokesh, Shende Dilip, Hussain Sana Yasmin, Srivastava Anurag, Seenu Vathulru
Department of Anesthesiology, Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi, India.
Department of Surgical Disciplines, All India Institute of Medical Sciences, New Delhi, India.
Saudi J Anaesth. 2020 Oct-Dec;14(4):464-472. doi: 10.4103/sja.SJA_822_19. Epub 2020 Sep 24.
Thoracic paravertebral block (TPVB) has become the gold standard to provide postoperative analgesia in breast surgery. Recently, ultrasound-guided (USG) pectoralis (PECS) block and serratus anterior plane (SAP) block have been described as an alternative to TPVB. The objectives were to compare TPVB, PECS, and SAP block in terms of analgesic efficacy and the spread of local anesthetic by ultrasound imaging, correlating it with the sensory blockade.
Prospective randomized interventional study conducted in 45 ASA grades I-II patients scheduled for the elective breast surgery. Patients were randomly allocated into three groups, i.e., Gr.1 (USG -TPVB) (ropivacaine 0.375% 20 ml), Gr.2 (USG-PECS II) block (ropivacaine 0.375% 30 ml), and Gr.3 (USG-SAP) (ropivacaine 0.375% 30 ml). Spread of the local anesthetics was seen with ultrasound imaging. Onset of sensory blockade, postoperative fentanyl consumption, and pain scores was measured.
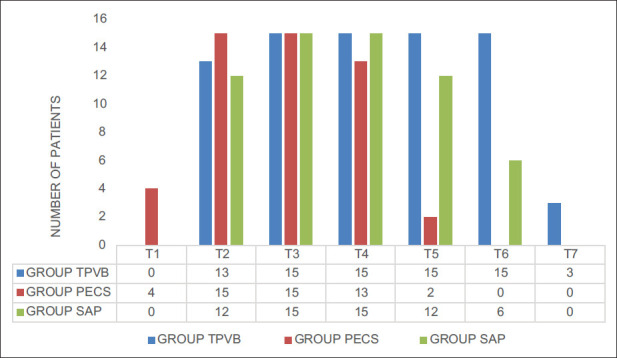
TPVB and SAP group had comparatively higher spread and sensory block compared to PECS group. Postoperative fentanyl requirement (mean ± SD) was 428.33 ± 243.1 μg, 644.67 ± 260.15 μg, and 415 ± 182.44 μg in the TPVB group, PECS II group, and SAP group, respectively. SAP group had significantly lesser requirement than PECS II group ( = 0.028) but similar requirement as in TPVB group ( = 1.0). Pain scores were not significantly different among the group in the postoperative period.
TPVB and SAP group result in a greater spread of the drug and provide equivalent analgesia and are superior to the PECS II block in providing analgesia for breast surgeries. SAP block is easier to perform than TPVB with lesser chances of complications and results in faster onset.
胸椎旁神经阻滞(TPVB)已成为乳腺手术术后镇痛的金标准。最近,超声引导下(USG)胸肌(PECS)阻滞和前锯肌平面(SAP)阻滞已被描述为TPVB的替代方法。目的是通过超声成像比较TPVB、PECS和SAP阻滞在镇痛效果和局麻药扩散方面的情况,并将其与感觉阻滞相关联。
对45例计划进行择期乳腺手术的ASA I-II级患者进行前瞻性随机干预研究。患者被随机分为三组,即第1组(USG-TPVB)(0.375%罗哌卡因20 ml)、第2组(USG-PECS II)阻滞(0.375%罗哌卡因30 ml)和第3组(USG-SAP)(0.375%罗哌卡因30 ml)。通过超声成像观察局麻药的扩散情况。测量感觉阻滞的起效时间、术后芬太尼消耗量和疼痛评分。
与PECS组相比,TPVB组和SAP组的局麻药扩散和感觉阻滞相对较高。TPVB组、PECS II组和SAP组术后芬太尼需求量(均值±标准差)分别为428.33±243.1μg、644.67±260.15μg和415±182.44μg。SAP组的需求量明显低于PECS II组(P = 0.028),但与TPVB组相似(P = 1.0)。术后各组疼痛评分无显著差异。
TPVB组和SAP组药物扩散范围更大,提供等效镇痛效果,在乳腺手术镇痛方面优于PECS II阻滞。SAP阻滞比TPVB更容易实施,并发症发生几率更小,起效更快。