Gulea Claudia, Zakeri Rosita, Quint Jennifer K
Department of Population Health, National Heart and Lung Institute, Imperial College London, London, UK.
NIHR Imperial Biomedical Research Centre, London, UK.
BMC Med. 2021 Jan 18;19(1):9. doi: 10.1186/s12916-020-01881-7.
Comorbidities affect outcomes in heart failure (HF), but are not reflected in current HF classification. The aim of this study is to characterize HF groups that account for higher-order interactions between comorbidities and to investigate the association between comorbidity groups and outcomes.
Latent class analysis (LCA) was performed on 12 comorbidities from patients with HF identified from administrative claims data in the USA (OptumLabs Data Warehouse®) between 2008 and 2018. Associations with admission to hospital and mortality were assessed with Cox regression. Negative binomial regression was used to examine rates of healthcare use.
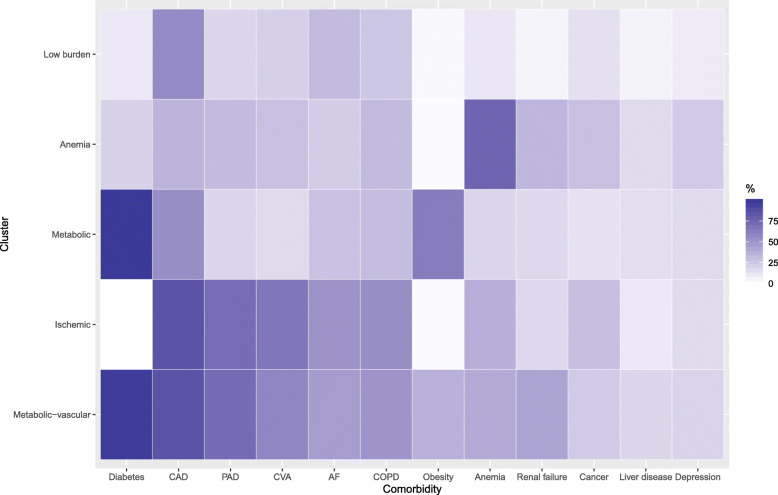
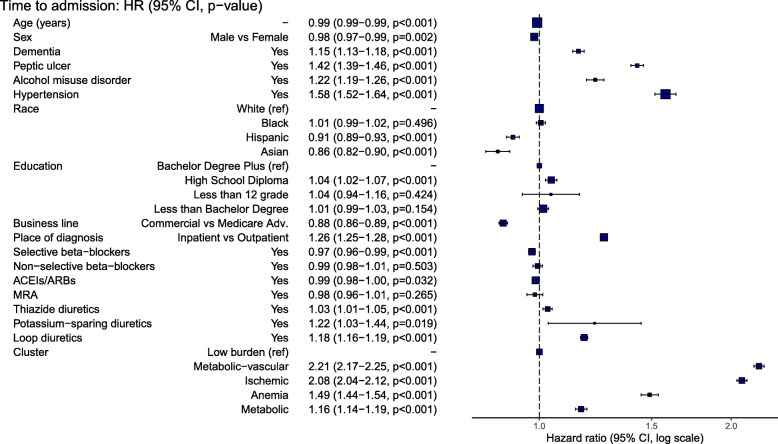
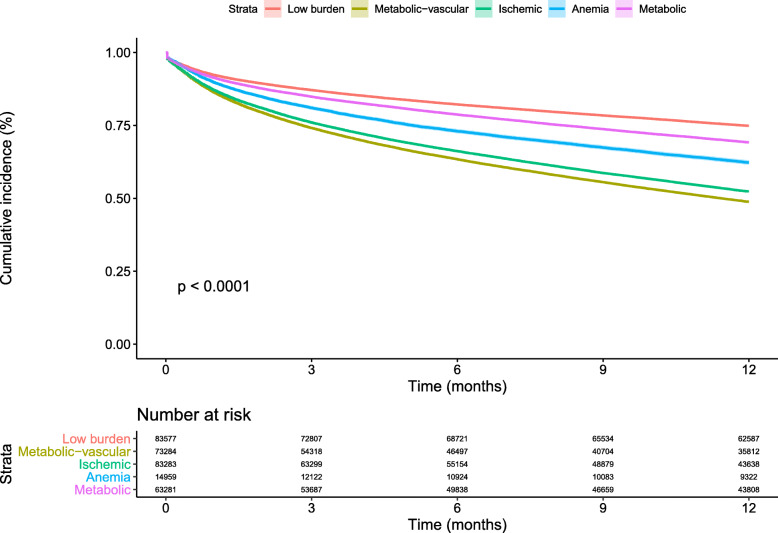
In a population of 318,384 individuals, we identified five comorbidity clusters, named according to their dominant features: low-burden, metabolic-vascular, anemic, ischemic, and metabolic. Compared to the low-burden group (minimal comorbidities), patients in the metabolic-vascular group (exhibiting a pattern of diabetes, obesity, and vascular disease) had the worst prognosis for admission (HR 2.21, 95% CI 2.17-2.25) and death (HR 1.87, 95% CI 1.74-2.01), followed by the ischemic, anemic, and metabolic groups. The anemic group experienced an intermediate risk of admission (HR 1.49, 95% CI 1.44-1.54) and death (HR 1.46, 95% CI 1.30-1.64). Healthcare use also varied: the anemic group had the highest rate of outpatient visits, compared to the low-burden group (IRR 2.11, 95% CI 2.06-2.16); the metabolic-vascular and ischemic groups had the highest rate of admissions (IRR 2.11, 95% CI 2.08-2.15, and 2.11, 95% CI 2.07-2.15) and healthcare costs.
These data demonstrate the feasibility of using LCA to classify HF based on comorbidities alone and should encourage investigation of multidimensional approaches in comorbidity management to reduce admission and mortality risk among patients with HF.
合并症会影响心力衰竭(HF)的预后,但目前的HF分类中并未体现这一点。本研究的目的是对合并症之间存在高阶相互作用的HF组进行特征描述,并调查合并症组与预后之间的关联。
对2008年至2018年期间从美国行政索赔数据(OptumLabs Data Warehouse®)中识别出的HF患者的12种合并症进行潜在类别分析(LCA)。采用Cox回归评估与住院和死亡率的关联。使用负二项回归来检查医疗保健使用率。
在318384名个体的人群中,我们识别出五个合并症集群,根据其主要特征命名为:低负担、代谢-血管、贫血、缺血和代谢。与低负担组(合并症最少)相比,代谢-血管组(表现出糖尿病、肥胖和血管疾病模式)的住院(风险比[HR] 2.21,95%置信区间[CI] 2.17 - 2.25)和死亡(HR 1.87,95% CI 1.74 - 2.01)预后最差,其次是缺血组、贫血组和代谢组。贫血组的住院(HR 1.49,95% CI 1.44 - 1.54)和死亡(HR 1.46,95% CI 1.30 - 1.64)风险处于中等水平。医疗保健使用情况也有所不同:与低负担组相比,贫血组的门诊就诊率最高(发病率比[IRR] 2.11,95% CI 2.06 - 2.16);代谢-血管组和缺血组的住院率(IRR 2.11,95% CI 2.08 - 2.15和2.11,95% CI 2.07 - 2.15)和医疗费用最高。
这些数据证明了仅基于合并症使用LCA对HF进行分类的可行性,并应鼓励对合并症管理中的多维方法进行研究,以降低HF患者的住院和死亡风险。