Wei Ning, Zhong Zhiheng, Shi Ruihua
Medical School of Southeast University, No. 87 Dingjiaqiao,, Nanjing, 210009, China.
Department of Gastroenterology, Southeast University Affiliated Zhongda Hospital, No. 87 Dingjiaqiao, Nanjing, 210009, China.
Cancer Cell Int. 2021 Jan 20;21(1):61. doi: 10.1186/s12935-021-01758-6.
Studies have shown the value of subtypes and distribution of gastric intestinal metaplasia (GIM) for prediction of gastric cancer. We aim to combine GIM subtypes and distribution to form a new scoring system for GIM.
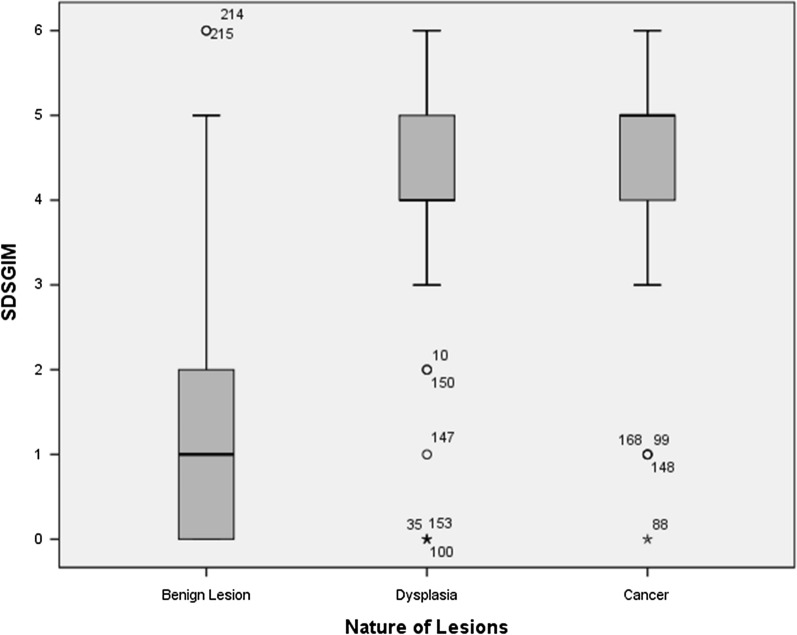
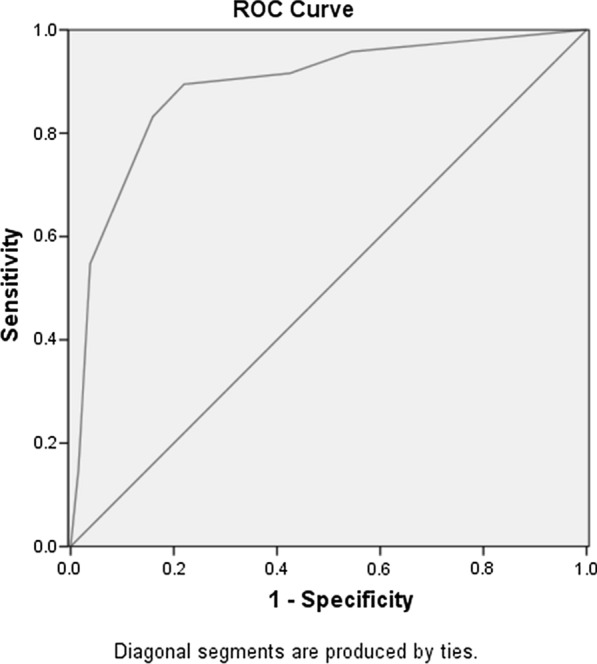
This was a cross-sectional study. No GIM, type I, II, and III GIM of gastric antrum and corpus scored 0-3 points respectively. Then the severity of the whole stomach was calculated in two ways: 1. The gastric antrum and corpus scores were added together, with a score ranging from 0 to 6, which named "Subtype Distribution Score of Gastric Intestinal Metaplasia (SDSGIM)". 2. Direct classification according to a table corresponding to that of OLGIM. We compared the SDSGIM among benign lesions, dysplasia, and cancer and drew receiver operating characteristic (ROC) curve to determine the optimal cut-off value. According to the cut-off value and the classification from the table, the predictive ability of these two methods were calculated.
227 patients were included. For SDSGIM, benign lesion group was significantly different from dysplasia or cancer group. Area under curve of ROC curve was 0.889 ± 0.023. The optimal cut-off value was 3. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of SDSGIM for malignancy were 89.5%, 78.0%, 74.6%, 91.2% and 82.8%. And those for the second classification method were 84.2%, 82.6%, 77.7%, 87.9%, and 83.3% respectively.
This study firstly combined GIM subtypes with its distribution forming a novel scoring system, which showed high prediction accuracy for malignant lesions.
研究表明胃化生(GIM)的亚型和分布对于预测胃癌具有重要价值。我们旨在将GIM亚型和分布结合起来,形成一种新的GIM评分系统。
这是一项横断面研究。胃窦和胃体的无GIM、I型、II型和III型GIM分别计0 - 3分。然后通过两种方式计算全胃的严重程度:1. 将胃窦和胃体的分数相加,得分范围为0至6分,称为“胃化生亚型分布评分(SDSGIM)”。2. 根据与OLGIM相对应的表格进行直接分类。我们比较了良性病变、发育异常和癌症之间的SDSGIM,并绘制了受试者工作特征(ROC)曲线以确定最佳截断值。根据截断值和表格中的分类,计算这两种方法的预测能力。
纳入227例患者。对于SDSGIM,良性病变组与发育异常或癌症组有显著差异。ROC曲线下面积为0.889±0.023。最佳截断值为3。SDSGIM对恶性肿瘤的敏感性、特异性、阳性预测值、阴性预测值和准确性分别为89.5%、78.0%、74.6%、91.2%和82.8%。而第二种分类方法的相应值分别为84.2%、82.6%、77.7%、87.9%和83.3%。
本研究首次将GIM亚型与其分布相结合,形成了一种新的评分系统,对恶性病变具有较高的预测准确性。