Second Department of Medicine and Nephrology-Diabetes Centre, University of Pécs Medical School, Pécs, Hungary.
RxTarget Ltd, Szolnok, Hungary.
BMJ Open Diabetes Res Care. 2021 Jan;9(1). doi: 10.1136/bmjdrc-2020-001765.
Mortality and disability in diabetes mellitus are determined mostly by cardiovascular complications and cancer. The impact of dipeptidyl peptidase-4 inhibitor (DPP-4i) and sodium-glucose cotransporter-2 inhibitor (SGLT2i) monotherapy or combination on long-term complications of type 2 diabetes mellitus was studied.
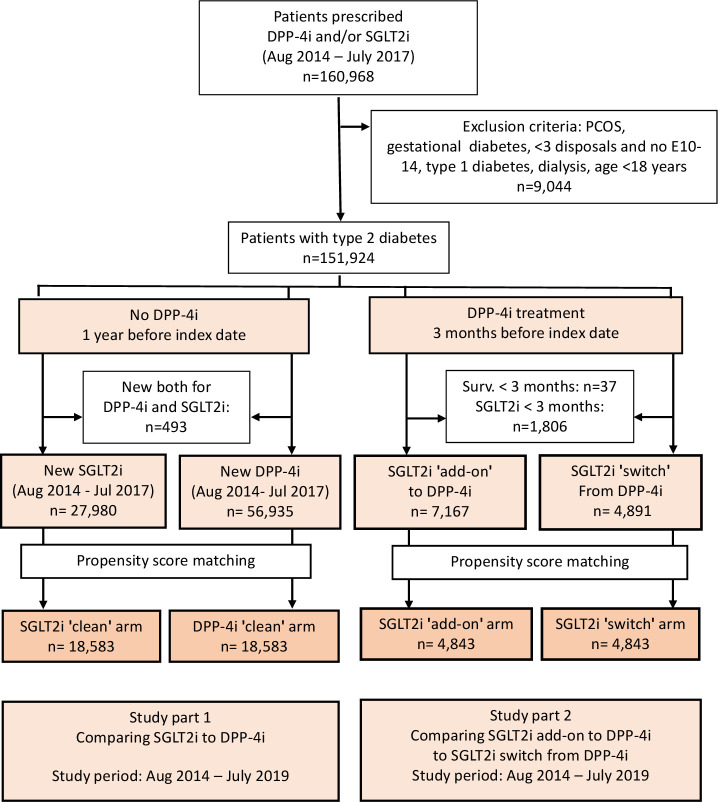
Patients with type 2 diabetes treated with DPP-4i or SGLT2i during a 3-year period were identified in the database of the National Institute of Health Insurance Fund in Hungary. All-cause mortality, acute myocardial infarction, stroke, hospitalization for heart failure (HHF), lower limb amputation (LLA) and cancer were assessed. Outcomes of add-on SGLT2i to DPP-4i treatment in comparison with switching DPP-4i therapy to SGLT2i were also evaluated. After propensity score matching, survival analysis was performed with a Cox proportional hazards model.
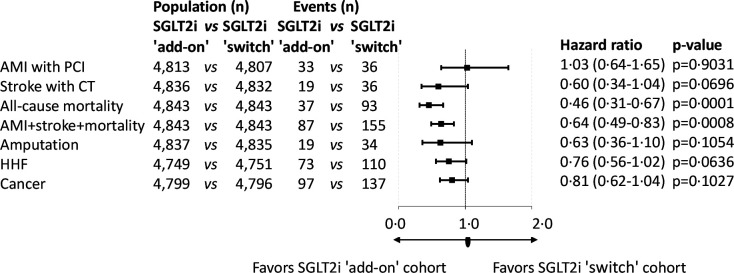
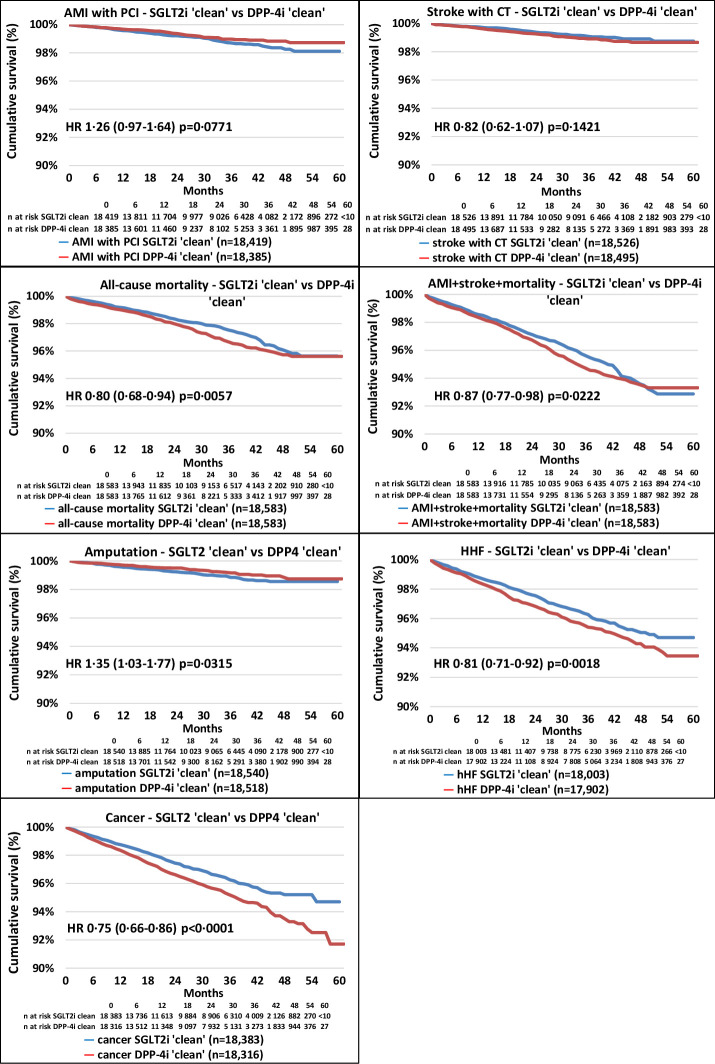
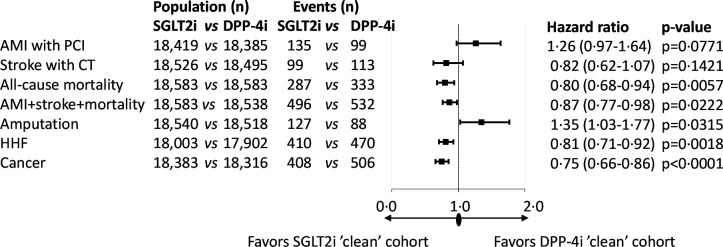
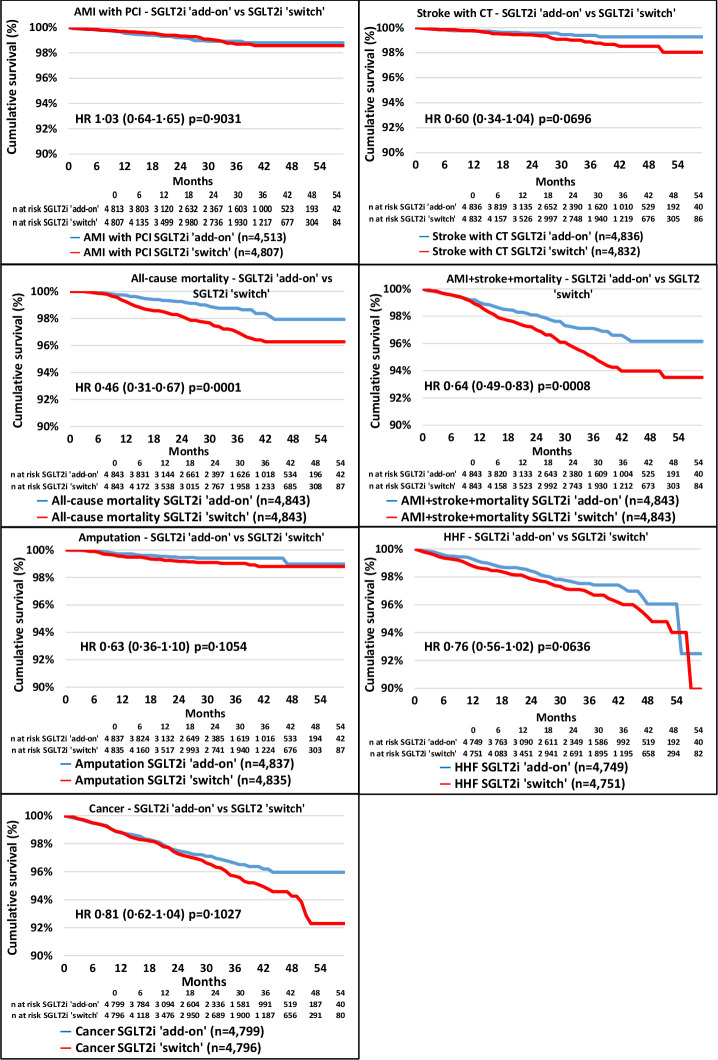
After propensity score matching, both SGLT2i and DPP-4i groups included 18 583 patients. All-cause mortality (HR, 0.80; 95% CI 0.68 to 0.94; p=0.0057), HHF (HR, 0.81; 95% CI 0.71 to 0.92; p=0.0018), and risk of cancer (HR, 0.75; 95% CI 0.66 to 0.86; p<0.0001) were lower in the SGLT2i population compared with DPP-4i. Risk of LLA was higher in the SGLT2i group (HR, 1.35; 95% CI 1.03 to 1.77; p=0.0315). SGLT2i in combination with DPP-4i results in lower all-cause mortality (HR, 0.46; 95% CI 0.31 to 0.67; p=0.0001), with a lower trend in stroke, LLA, HHF and cancer, but without any statistical difference.
SGLT2i treatment leads to a lower risk of overall mortality, HHF and cancer when compared with DPP-4i treatment. Adding SGLT2i to DPP-4i instead of switching from DPP-4i to SGLT2i further lowers the risk of all-cause mortality.
糖尿病的死亡率和失能率主要由心血管并发症和癌症决定。本研究旨在探讨二肽基肽酶-4 抑制剂(DPP-4i)和钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)单药或联合治疗对 2 型糖尿病长期并发症的影响。
在匈牙利国家健康保险基金数据库中,确定了在 3 年内接受 DPP-4i 或 SGLT2i 治疗的 2 型糖尿病患者。评估了全因死亡率、急性心肌梗死、卒中和心力衰竭住院(HHF)、下肢截肢(LLA)和癌症。还评估了在 DPP-4i 治疗中添加 SGLT2i 与将 DPP-4i 治疗转换为 SGLT2i 相比的治疗效果。在进行倾向评分匹配后,使用 Cox 比例风险模型进行生存分析。
在进行倾向评分匹配后,SGLT2i 和 DPP-4i 组各纳入 18583 例患者。与 DPP-4i 组相比,SGLT2i 组的全因死亡率(HR,0.80;95%CI 0.68 至 0.94;p=0.0057)、HHF(HR,0.81;95%CI 0.71 至 0.92;p=0.0018)和癌症风险(HR,0.75;95%CI 0.66 至 0.86;p<0.0001)均较低。SGLT2i 组的 LLA 风险较高(HR,1.35;95%CI 1.03 至 1.77;p=0.0315)。SGLT2i 与 DPP-4i 联合使用可降低全因死亡率(HR,0.46;95%CI 0.31 至 0.67;p=0.0001),并呈降低卒中、LLA、HHF 和癌症的趋势,但无统计学差异。
与 DPP-4i 治疗相比,SGLT2i 治疗可降低全因死亡率、HHF 和癌症风险。在 DPP-4i 治疗中添加 SGLT2i 而非将其转换为 SGLT2i 可进一步降低全因死亡率风险。