M&S Decisions LLC, Moscow, Russia.
Clinical Pharmacology & Quantitative Pharmacology, Clinical Pharmacology & Safety Sciences, R&D, AstraZeneca, Gothenburg, Sweden.
Int J Chron Obstruct Pulmon Dis. 2021 Jan 15;16:101-111. doi: 10.2147/COPD.S284720. eCollection 2021.
Lung function, measured as forced expiratory volume in one second (FEV), and exacerbations are two endpoints evaluated in chronic obstructive pulmonary disease (COPD) clinical trials. Joint analysis of these endpoints could potentially increase statistical power and enable assessment of efficacy in shorter and smaller clinical trials.
To evaluate joint modelling as a tool for analyzing treatment effects in COPD clinical trials by quantifying the association between longitudinal improvements in FEV and exacerbation risk reduction.
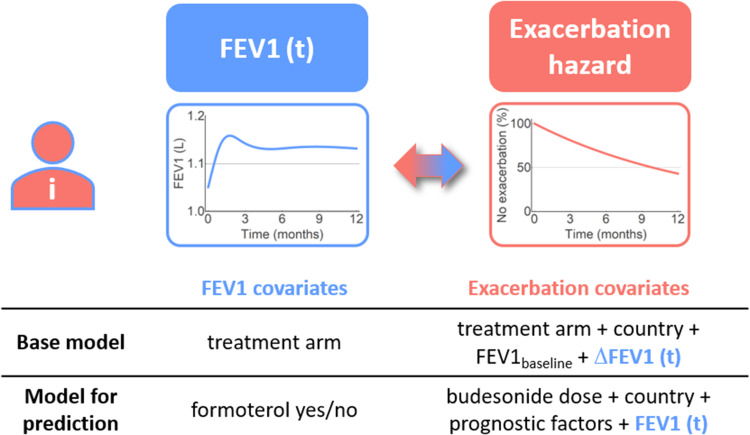
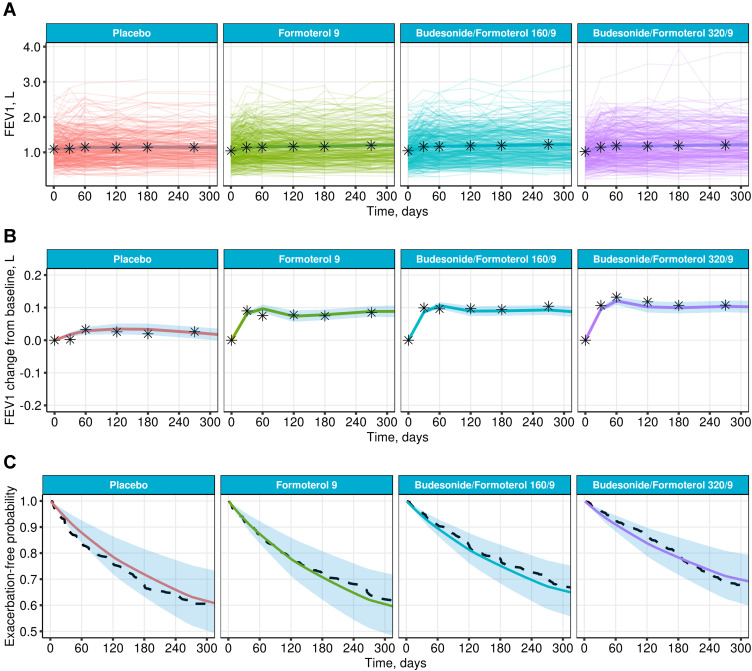
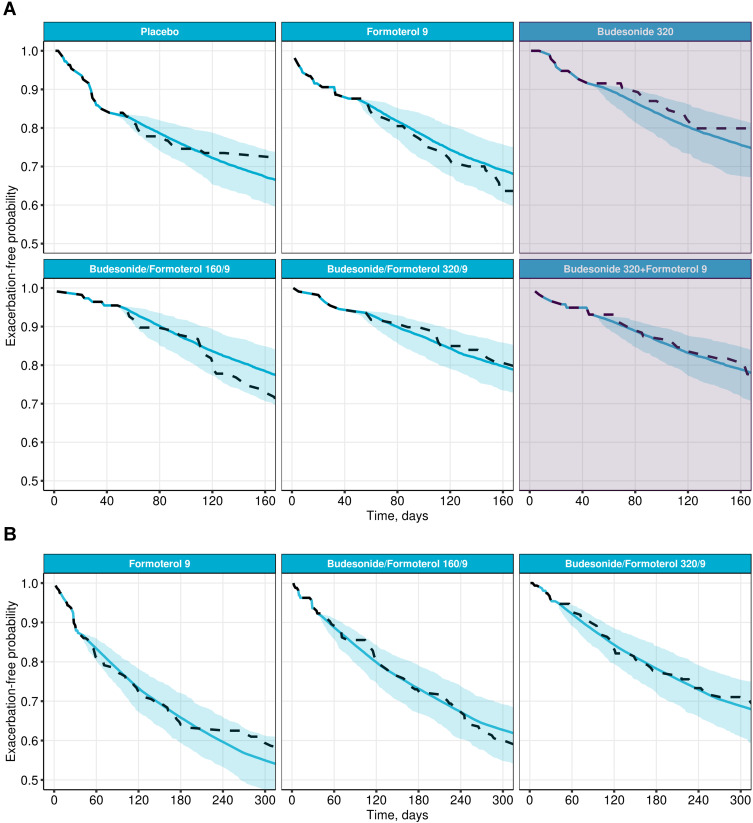
A joint model of longitudinal FEV and exacerbation risk was developed based on patient-level data from a Phase III clinical study in moderate-to-severe COPD (1740 patients), evaluating efficacy of fixed-dose combinations of a long-acting bronchodilator, formoterol, and an inhaled corticosteroid, budesonide. Two additional studies (1604 and 1042 patients) were used for external model validation and parameter re-estimation.
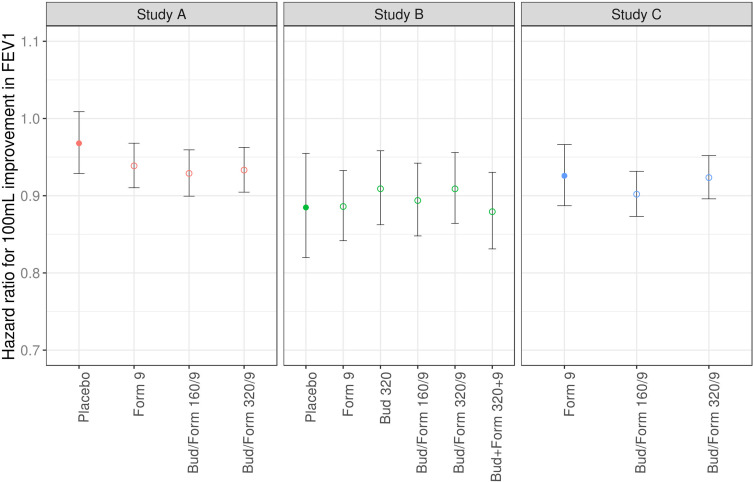
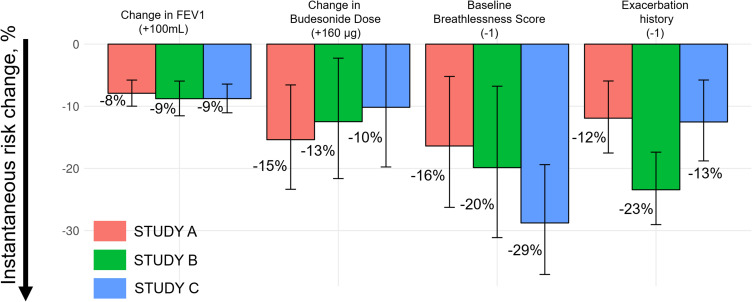
A significant (p<0.0001) association between FEV and exacerbation risk was estimated, with an approximate 10% reduction in exacerbation risk per 100 mL improvement in FEV, consistent across trials and treatment arms. The risk reduction associated with improvements in FEV was relatively small compared to the overall exacerbation risk reduction for treatment arms including budesonide (10-15% per 160 µg budesonide). High baseline breathlessness score and previous history of exacerbations also influenced the risk of exacerbation.
Joint modelling can be used to co-analyze longitudinal FEV and exacerbation data in COPD clinical trials. The association between the endpoints was consistent and appeared unrelated to treatment mechanism, suggesting that improved lung function is indicative of an exacerbation risk reduction. The risk reduction associated with improved FEV was, however, generally small and no major impact on exacerbation trial design can be expected based on FEV alone. Further exploration with other longitudinal endpoints should be considered to further evaluate the use of joint modelling in analyzing COPD clinical trials.
在慢性阻塞性肺疾病(COPD)临床试验中,肺功能(以一秒用力呼气量(FEV)衡量)和加重是两个评估终点。联合分析这些终点可能会增加统计学效力,并能够在更短、更小的临床试验中评估疗效。
通过量化 FEV 纵向改善与加重风险降低之间的关联,评估联合模型作为 COPD 临床试验中分析治疗效果的工具。
基于中度至重度 COPD 的 III 期临床试验(1740 例患者)的患者水平数据,开发了一个 FEV 和加重风险的联合模型,该试验评估了长效支气管扩张剂福莫特罗和吸入性皮质类固醇布地奈德固定剂量组合的疗效。另外两项研究(1604 例和 1042 例患者)用于外部模型验证和参数重新估计。
FEV 和加重风险之间存在显著关联(p<0.0001),FEV 每改善 100 mL,加重风险降低约 10%,在所有试验和治疗组中一致。与包括布地奈德在内的治疗组(每 160 µg 布地奈德降低 10-15%)的总体加重风险降低相比,与 FEV 改善相关的风险降低相对较小。基线呼吸困难评分高和既往加重史也会影响加重的风险。
联合模型可用于 COPD 临床试验中对 FEV 和加重数据进行联合分析。终点之间的关联是一致的,并且与治疗机制无关,这表明肺功能改善预示着加重风险降低。然而,与 FEV 改善相关的风险降低通常较小,不能仅基于 FEV 对加重试验设计产生重大影响。应进一步探索其他纵向终点,以进一步评估联合模型在分析 COPD 临床试验中的应用。