Goodsmith Nichole, Zhang Lily, Ong Michael K, Ngo Victoria K, Miranda Jeanne, Hirsch Susan, Jones Felica, Wells Kenneth, Chung Bowen
U.S. Department of Veterans Affairs (VA) Center for the Study of Healthcare Innovation, Implementation, and Policy (Goodsmith) and Department of Medicine (Ong), VA Greater Los Angeles Healthcare System, Los Angeles; National Clinician Scholars Program (Goodsmith), Department of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine (Zhang, Miranda, Hirsch), Division of General Internal Medicine and Health Services Research, David Geffen School of Medicine (Ong), Department of Health Policy and Management, Jonathan and Karin Fielding School of Public Health (Miranda), and Center for Health Services and Society, Jane and Terry Semel Institute for Neuroscience and Human Behavior (Wells, Chung), University of California, Los Angeles; Graduate School of Public Health and Health Policy, City University of New York, New York City (Ngo); RAND Corporation, Santa Monica, California (Ngo, Wells); Healthy African American Families II, Los Angeles (Jones); County of Los Angeles Department of Mental Health, Los Angeles (Chung).
Psychiatr Serv. 2021 Mar 1;72(3):281-287. doi: 10.1176/appi.ps.202000095. Epub 2021 Jan 27.
Suicidality is common among participants in clinical trials and health services research, but approaches to suicide risk assessment and mitigation vary widely. Studies involving vulnerable populations with limited access to care raise additional ethical concerns. The authors applied a community-partnered approach to develop and implement a suicide-risk management protocol (SRMP) in a depression study in an underresourced setting in Los Angeles.
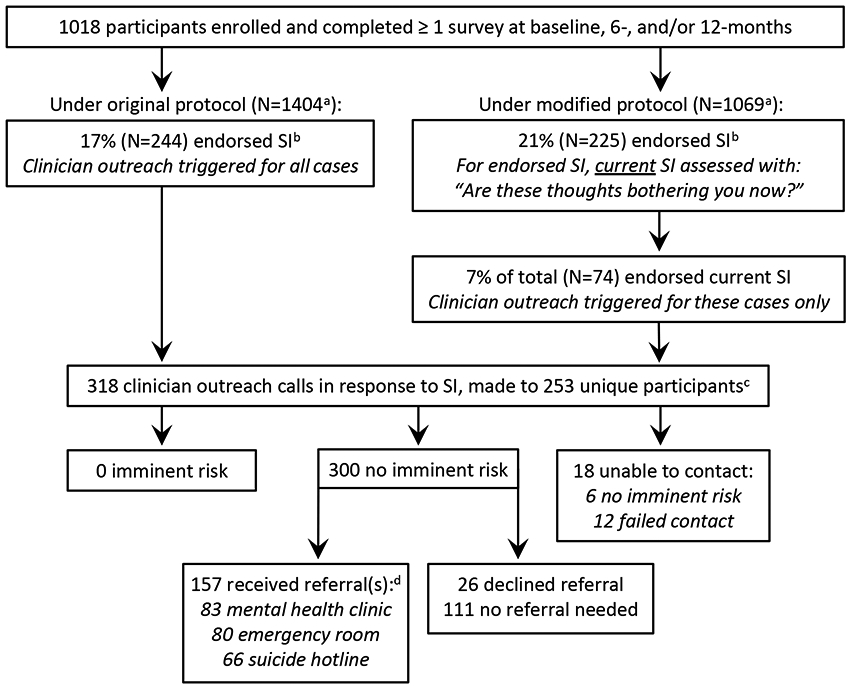
Using a community-partnered participatory research framework, the authors designed and adapted the SRMP. Qualitative data regarding SRMP implementation included notes from SRMP development meetings and from study clinicians conducting outreach calls to study participants. Analyses included baseline and 6- and 12-month telephone survey data from 1,018 enrolled adults with moderate to severe depressive symptoms (8-item Patient Health Questionnaire score ≥10), of whom 48% were Black and 40% Latino.
Community stakeholders prioritized a robust SRMP to ensure participant safety. Features included rapid telephone outreach by study clinicians in all cases of reported recent suicidality and expedited treatment access. Using a suicidality timeframe prompt of "in the past 2 weeks," endorsement of suicidality was common (15% at baseline, 32% cumulative). Midway through the study, the SRMP was modified to assess for present suicidality, which reduced the frequency of clinician involvement. Overall, 318 outreach calls were placed, with none requiring an emergency response. Treatment referrals were provided in 157 calls, and outreach was well received.
SRMP implementation in research involving underresourced and vulnerable communities merits additional considerations. Partnering with community stakeholders can facilitate the development of acceptable and feasible SRMP procedures.
自杀倾向在临床试验和卫生服务研究的参与者中很常见,但自杀风险评估和缓解方法差异很大。涉及难以获得医疗服务的弱势群体的研究引发了更多伦理问题。作者采用社区合作方法,在洛杉矶资源匮乏地区的一项抑郁症研究中制定并实施了自杀风险管理协议(SRMP)。
作者使用社区合作参与式研究框架设计并调整了SRMP。关于SRMP实施的定性数据包括SRMP制定会议的记录以及研究临床医生给研究参与者打外联电话的记录。分析包括来自1018名登记的有中度至重度抑郁症状(8项患者健康问卷得分≥10)的成年人的基线以及6个月和12个月的电话调查数据,其中48%为黑人,40%为拉丁裔。
社区利益相关者将强大的SRMP列为确保参与者安全的优先事项。其特点包括在所有报告近期有自杀倾向的情况下,研究临床医生迅速进行电话外联并加快治疗途径。使用“过去两周内”的自杀倾向时间框架提示,自杀倾向的认可很常见(基线时为15%,累计为32%)。在研究进行到一半时,SRMP被修改为评估当前的自杀倾向,这减少了临床医生介入的频率。总体而言,共拨打了318次外联电话,无一需要紧急响应。在157次电话中提供了治疗转诊,外联工作受到好评。
在涉及资源匮乏和弱势群体的研究中实施SRMP值得进一步考虑。与社区利益相关者合作可以促进制定可接受且可行的SRMP程序。