McGonagle Dennis, Bridgewood Charlie, Ramanan Athimalaipet V, Meaney James F M, Watad Abdulla
Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, UK.
National Institute for Health Research Leeds Biomedical Research Centre, Leeds Teaching Hospitals, Leeds, UK.
Lancet Rheumatol. 2021 Mar;3(3):e224-e233. doi: 10.1016/S2665-9913(20)30420-3. Epub 2021 Jan 7.
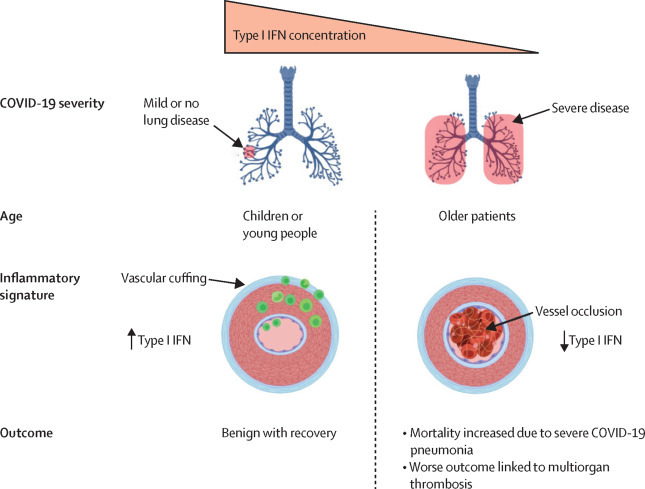
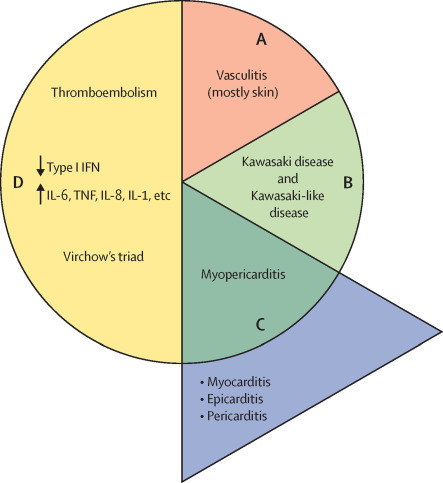
COVID-19 has been occasionally linked to histologically confirmed cutaneous vasculitis and a Kawasaki-like vasculitis, with these entities generally having minimal or no lung involvement and a good prognosis. Unlike these vasculitis types, patients with severe COVID-19 pneumonia can develop cutaneous vasculitis-like lesions and systemic arterial and venous thromboemboli, including cryptogenic strokes and other vasculopathy features. Proposed underlying mechanisms for these severe manifestations have encompassed immune dysregulation, including an anti-phospholipid syndrome-like state, complement activation, viral dissemination with direct systemic endothelial infection, viral RNAaemia with immunothrombosis, clotting pathway activation mediated by hypoxaemia, and immobility. In this Viewpoint, we highlight how imaging and post-mortem findings from patients with COVID-19 indicate a novel thrombosis in the pulmonary venous territory distal to the alveolar capillary bed, a territory that normally acts as a clot filtration system, which might represent an unappreciated nidus for systemic microembolism. Additionally, we suggest that this mechanism represents a novel vasculitis mimic related to COVID-19 that might lead to cryptogenic strokes across multivessel territories, acute kidney injury with haematuria, a skin vasculitis mimic, intestinal ischaemia, and other organ ischaemic manifestations. This finding is supported by pathological reports of extensive pulmonary venular thrombosis and peripheral organ thrombosis with pauci-immune cellular infiltrates. Therefore, severe COVID-19 pneumonia with extensive pulmonary intravascular coagulopathy might help to explain the numerous systemic complications of COVID-19, in which the demonstration of direct organ infection has not adequately explained the pathology.
新型冠状病毒肺炎(COVID-19)偶尔与组织学确诊的皮肤血管炎和川崎样血管炎相关,这些疾病通常肺部受累轻微或无肺部受累,预后良好。与这些血管炎类型不同,重症COVID-19肺炎患者可出现皮肤血管炎样病变以及系统性动脉和静脉血栓栓塞,包括隐源性卒中及其他血管病变特征。针对这些严重表现提出的潜在机制包括免疫失调,如抗磷脂综合征样状态、补体激活、病毒播散伴直接系统性内皮感染、病毒血症伴免疫性血栓形成、低氧血症介导的凝血途径激活以及制动。在本观点文章中,我们强调COVID-19患者的影像学和尸检结果如何表明在肺泡毛细血管床远端的肺静脉区域存在一种新型血栓形成,该区域通常作为凝血过滤系统,可能是系统性微栓塞未被认识的病灶。此外,我们认为这一机制代表了一种与COVID-19相关的新型血管炎模拟物,可能导致多血管区域的隐源性卒中、血尿性急性肾损伤、皮肤血管炎模拟物、肠道缺血及其他器官缺血表现。广泛肺静脉血栓形成和伴有少量免疫细胞浸润的外周器官血栓形成的病理报告支持了这一发现。因此,伴有广泛肺内凝血病变的重症COVID-19肺炎可能有助于解释COVID-19众多的全身并发症,而直接器官感染的证据并不能充分解释这些病理情况。