Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA, United States of America.
Clinical and Translational Epidemiology Unit, Massachusetts General Hospital and Harvard Medical School, Boston, MA, United States of America.
PLoS Med. 2021 Feb 1;18(2):e1003522. doi: 10.1371/journal.pmed.1003522. eCollection 2021 Feb.
Healthy lifestyle and screening represent 2 major approaches to colorectal cancer (CRC) prevention. It remains unknown whether the CRC-preventive benefit of healthy lifestyle differs by endoscopic screening status, and how the combination of healthy lifestyle with endoscopic screening can improve CRC prevention.
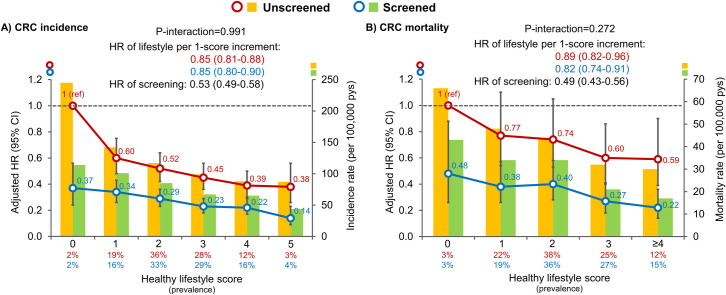
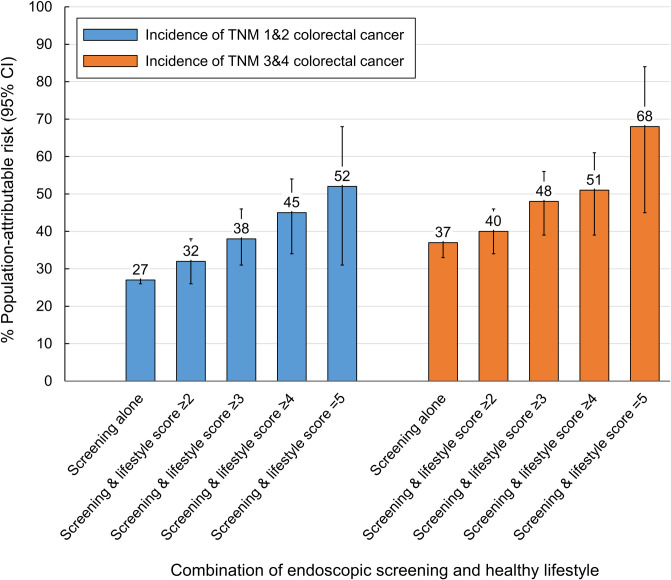
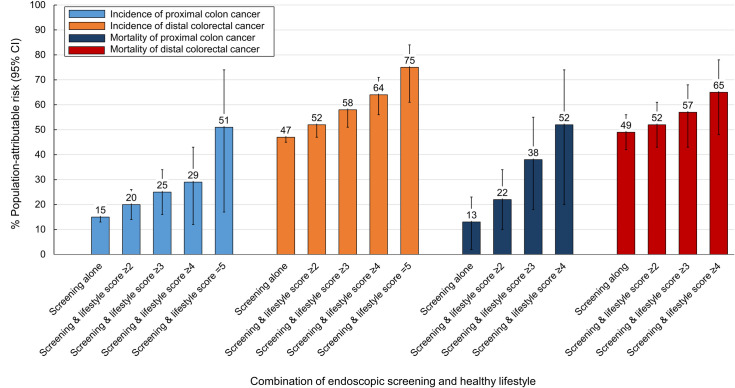
We assessed lifestyle and endoscopic screening biennially among 75,873 women (Nurses' Health Study, 1988 to 2014) and 42,875 men (Health Professionals Follow-up Study, 1988 to 2014). We defined a healthy lifestyle score based on body mass index, smoking, physical activity, alcohol consumption, and diet. We calculated hazard ratios (HRs) and population-attributable risks (PARs) for CRC incidence and mortality in relation to healthy lifestyle score according to endoscopic screening. Participants' mean age (standard deviation) at baseline was 54 (8) years. During a median of 26 years (2,827,088 person-years) follow-up, we documented 2,836 incident CRC cases and 1,013 CRC deaths. We found a similar association between healthy lifestyle score and lower CRC incidence among individuals with and without endoscopic screening, with the multivariable HR per one-unit increment of 0.85 (95% CI, 0.80 to 0.90) and 0.85 (95% CI, 0.81 to 0.88), respectively (P-interaction = 0.99). The fraction of CRC cases that might be prevented (PAR) by endoscopic screening alone was 32% (95% CI, 31% to 33%) and increased to 61% (95% CI, 42% to 75%) when combined with healthy lifestyle (score = 5). The corresponding PAR (95% CI) increased from 15% (13% to 16%) to 51% (17% to 74%) for proximal colon cancer and from 47% (45% to 50%) to 75% (61% to 84%) for distal CRC. Results were similar for CRC mortality. A limitation of our study is that our study participants are all health professionals and predominantly whites, which may not be representative of the general population.
Our study suggests that healthy lifestyle is associated with lower CRC incidence and mortality independent of endoscopic screening. An integration of healthy lifestyle with endoscopic screening may substantially enhance prevention for CRC, particularly for proximal colon cancer, compared to endoscopic screening alone.
健康的生活方式和筛查是预防结直肠癌(CRC)的两种主要方法。目前尚不清楚健康生活方式对 CRC 的预防作用是否因内镜筛查状况而异,以及健康生活方式与内镜筛查相结合如何提高 CRC 的预防效果。
我们在 75873 名女性(护士健康研究,1988 年至 2014 年)和 42875 名男性(健康专业人员随访研究,1988 年至 2014 年)中每两年评估一次生活方式和内镜筛查。我们根据身体质量指数、吸烟、体力活动、饮酒和饮食定义了健康生活方式评分。我们根据内镜筛查结果计算了 CRC 发病率和死亡率与健康生活方式评分之间的风险比(HR)和人群归因风险(PAR)。参与者的基线平均年龄(标准差)为 54(8)岁。在中位 26 年(2827088 人年)的随访期间,我们记录了 2836 例 CRC 病例和 1013 例 CRC 死亡。我们发现,在有内镜筛查和无内镜筛查的个体中,健康生活方式评分与较低的 CRC 发病率之间存在相似的关联,多变量 HR 分别为 0.85(95%CI,0.80 至 0.90)和 0.85(95%CI,0.81 至 0.88)(P 交互=0.99)。单独进行内镜筛查可预防的 CRC 病例比例(PAR)为 32%(95%CI,31%至 33%),与健康生活方式(评分=5)相结合时增加到 61%(95%CI,42%至 75%)。近端结肠癌的相应 PAR(95%CI)从 15%(13%至 16%)增加到 51%(17%至 74%),远端 CRC 从 47%(45%至 50%)增加到 75%(61%至 84%)。CRC 死亡率的结果相似。我们研究的一个局限性是我们的研究参与者都是健康专业人员,而且主要是白人,这可能不能代表一般人群。
我们的研究表明,健康的生活方式与独立于内镜筛查的 CRC 发病率和死亡率降低有关。与单独进行内镜筛查相比,将健康生活方式与内镜筛查相结合可以显著提高 CRC 的预防效果,特别是对近端结肠癌。