Eskisehir City Hospital, Department of Cardiology, Eskisehir, Turkey.
Eskisehir City Hospital, Department of Emergency Medicine, Eskisehir, Turkey.
Heart Lung. 2021 Mar-Apr;50(2):329-333. doi: 10.1016/j.hrtlng.2021.01.016. Epub 2021 Jan 26.
Coronavirus disease 2019 (COVID-19) has become a global health threat, and thus, an early and effective set of predictors is needed to manage the course of the disease.
We aim to determine the effect of SARS-CoV-2 on lipid profile and to evaluate whether the atherogenic index of plasma (AIP) could be used to predict in-hospital mortality in COVID-19 patients.
In this retrospective chart review study, a total of 139 confirmed COVID-19 patients, whose diagnoses are confirmed by PCR and computerized tomography results, are enrolled. The study population is divided into two groups: the deceased patient group and the survivor group. For each patient, fasting total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) and the triglyceride values are obtained from the laboratory tests required at the admission to hospital. Finally, the AIP is calculated as the base 10 logarithm of the triglyceride to HDL-C ratio. Distributional normality of the data is checked and depending on the normality of the data, either T test or Mann Whithey U test is employed to compare the two aforementioned study groups.
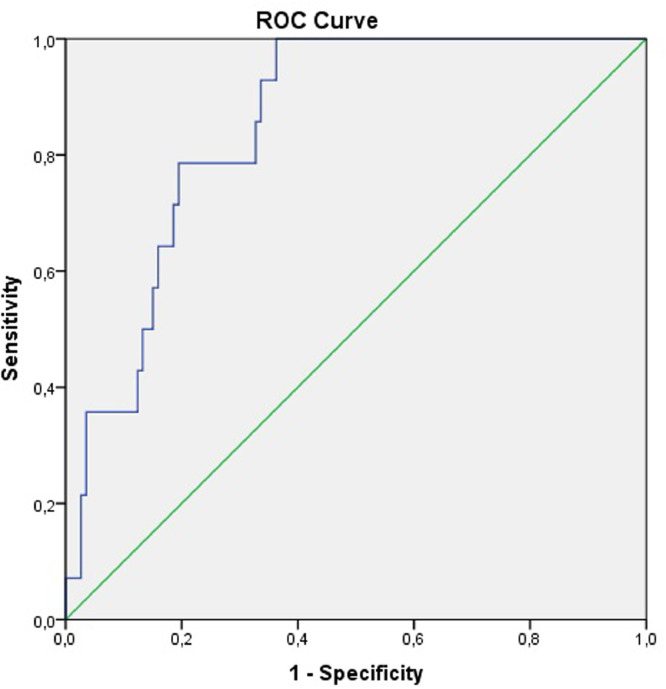
Mean age of the study population is 49.2 ± 20.8 and 61.2% (n = 85) is male. Out of the 139 patients 26 have deceased and the remaining 113 patients survived the disease. Mean age of the deceased patients was 71.88.9 and mean age of the survivor patients is 44.019.2 (p < 0.001). The deceased group had more patients with hypertension (50.0% vs. 23.0, p = 0.006), diabetes mellitus (35.6% vs. 10.6%, p = 0.002), cardiovascular diseases (23.1% vs. 4.4%, p = 0.001), chronic renal insufficiency (11.5% vs. 0.9%, p = 0.003) and atrial fibrillation (7.7% vs 0%, p = 0.003). The AIP values in the deceased group are found to be statistically higher (p < 0.001) than the survivor group. As a measure of mortality, the area under the operating characteristic curve for the AIP is calculated as 0.850 (95% confidence interval: 0.772-0.928) along with the optimal cut-off value of 0.6285 (78.6% sensitivity and 80.5% specificity). Furthermore, the AIP value is observed to be elevated in patients with pneumonia, intubation history, and intensive care admission during hospital stay (p = 0.002, p < 0.001 and p < 0.001, respectively). Finally, compared to the survivor group, total cholesterol, HDL-C, LDL-C values are lower (p = 0.004, p < 0.001 and p < 0.001, respectively) and triglyceride levels are higher (p < 0.001) in deceased patients.
In this study, we show that the AIP levels higher than 0.6285 can predict in-hospital mortality for COVID-19 patients. Moreover, the AIP emerges as a good candidate to be used as an early biomarker to predict pneumonia, intubation and intensive care need. Hence, regular check of the AIP levels in COVID-19 patients can improve management of these patients and prevent deterioration of the disease.
2019 年冠状病毒病(COVID-19)已成为全球健康威胁,因此,需要及早有效地确定一组预测指标来管理疾病进程。
我们旨在确定 SARS-CoV-2 对血脂谱的影响,并评估载脂蛋白指数(AIP)是否可用于预测 COVID-19 患者的住院死亡率。
在这项回顾性图表审查研究中,共纳入了 139 例经 PCR 和计算机断层扫描结果确诊的 COVID-19 患者。研究人群分为两组:死亡患者组和幸存者组。对于每个患者,从入院时进行的实验室检查中获得空腹总胆固醇、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)和甘油三酯值。最后,通过将甘油三酯与 HDL-C 的比值取以 10 为底的对数来计算 AIP。检查数据的分布正态性,根据数据的正态性,使用 T 检验或曼惠特尼 U 检验比较上述两个研究组。
研究人群的平均年龄为 49.2±20.8,61.2%(n=85)为男性。139 例患者中,26 例死亡,其余 113 例幸存。死亡患者的平均年龄为 71.88.9,幸存者患者的平均年龄为 44.019.2(p<0.001)。死亡组中高血压患者比例较高(50.0%比 23.0%,p=0.006),糖尿病患者比例较高(35.6%比 10.6%,p=0.002),心血管疾病患者比例较高(23.1%比 4.4%,p=0.001),慢性肾功能不全患者比例较高(11.5%比 0.9%,p=0.003),心房颤动患者比例较高(7.7%比 0%,p=0.003)。死亡组的 AIP 值明显高于幸存者组(p<0.001)。作为死亡率的衡量指标,AIP 的接受者操作特征曲线下面积计算为 0.850(95%置信区间:0.772-0.928),最佳截断值为 0.6285(78.6%的敏感性和 80.5%的特异性)。此外,在住院期间患有肺炎、有插管史和入住重症监护病房的患者中,AIP 值升高(p=0.002,p<0.001 和 p<0.001)。最后,与幸存者组相比,死亡组患者的总胆固醇、HDL-C 和 LDL-C 值较低(p=0.004,p<0.001 和 p<0.001),甘油三酯水平较高(p<0.001)。
在这项研究中,我们表明 AIP 水平高于 0.6285 可以预测 COVID-19 患者的住院死亡率。此外,AIP 可以作为预测肺炎、插管和需要重症监护的早期生物标志物。因此,定期检查 COVID-19 患者的 AIP 水平可以改善这些患者的管理,并防止病情恶化。