Pandey Ritu, Johnson Nathan, Cooke Laurence, Johnson Benny, Chen Yuliang, Pandey Manjari, Chandler Jason, Mahadevan Daruka
Cancer Center, University of Arizona, Tucson, AZ 85724, USA.
Department of Cellular and Molecular Medicine, University of Arizona, Tucson, AZ 85724, USA.
Cancers (Basel). 2021 Feb 3;13(4):597. doi: 10.3390/cancers13040597.
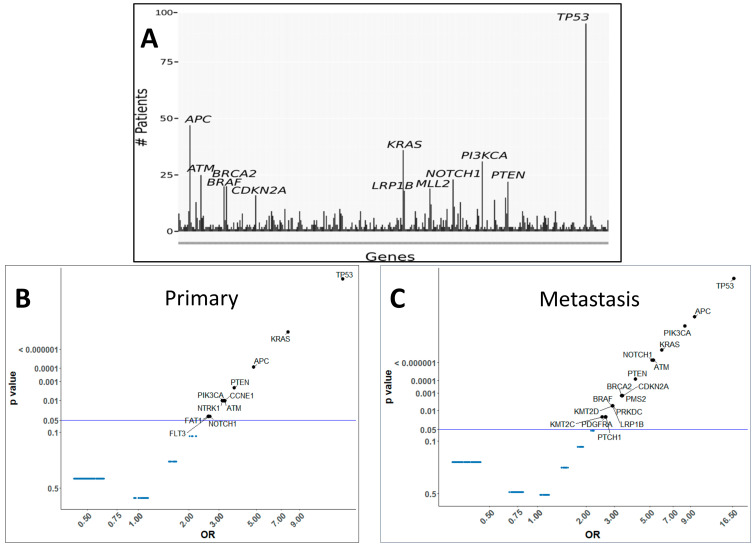
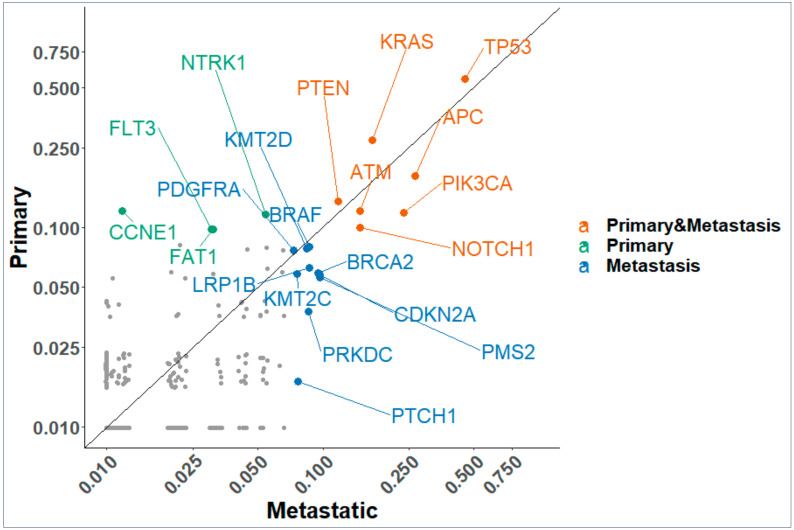
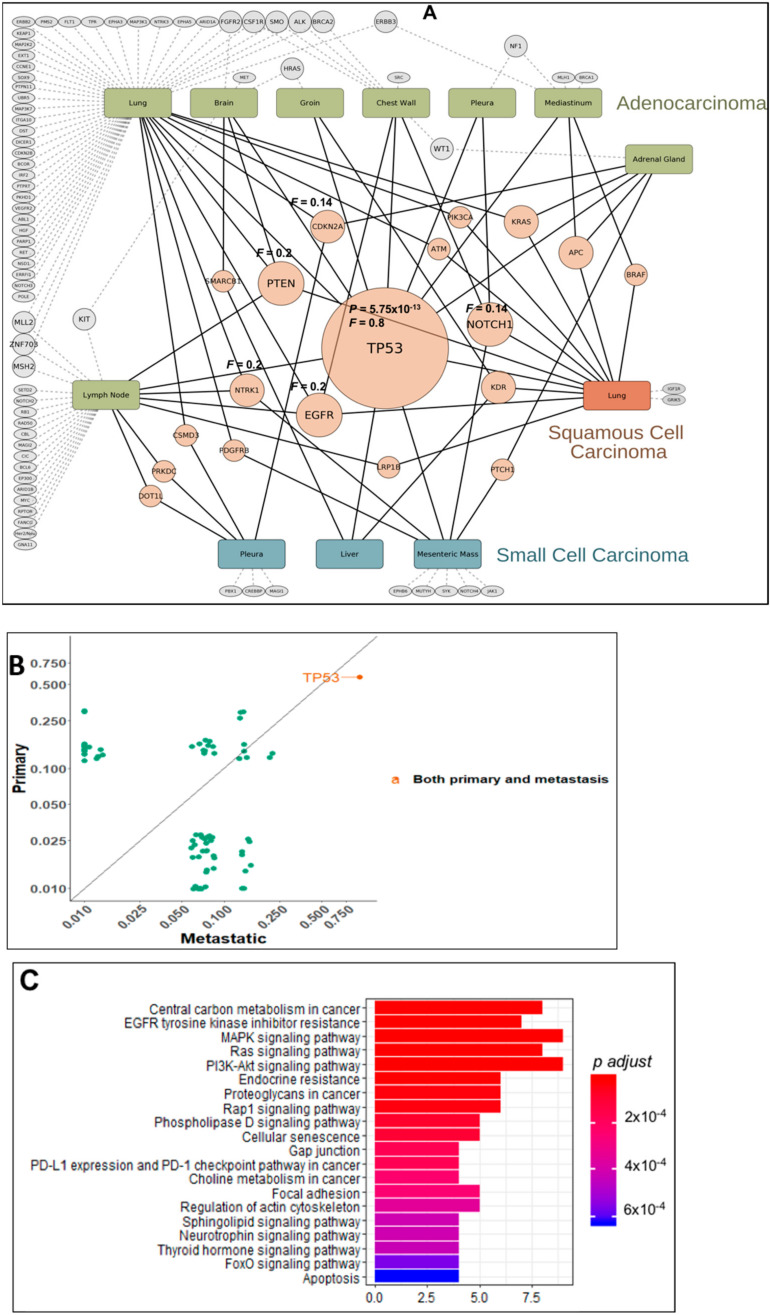
Molecular profiling with next generation sequencing (NGS) delivers key information on mutant gene sequences, copy number alterations, gene-fusions, and with immunohistochemistry (IHC), is a valuable tool in clinical decision making for patients entering investigational agent trials. Our objective was to elucidate mutational profiles from primary versus metastatic sites from advanced cancer patients to guide rational therapy. All phase I patients ( = 203) with advanced cancer were profiled by commercially available NGS platforms. The samples were annotated by histology, primary and metastatic site, biopsy site, gene mutations, mutation count/gene, and mutant . A molecular profile of each patient was categorized into common and unique mutations, signaling pathways for each profile and mutations mapped to 3D-structure of p53 bound to DNA and pre/post therapy molecular response. Of the 171 patients analyzed, 145 had genetic alterations from primary and metastatic sites. The predominant histology was adenocarcinoma followed by squamous cell carcinoma, carcinoma of unknown primary site (CUPS), and melanoma. Of 790 unique mutations, is the most common followed by , , , , , , , , , , and was found in most metastatic sites and appears to be a key driver of acquired drug resistance. We highlight examples of acquired mutational profiles pre-/post- targeted therapy in multiple tumor types with a menu of potential targeted agents. Conclusion: The mutational profiling of primary and metastatic lesions in cancer patients provides an opportunity to identify driver 'pathways' that may predict for drug sensitivity/resistance and guide rational drug combinations in clinical trials.
通过下一代测序(NGS)进行分子谱分析可提供有关突变基因序列、拷贝数改变、基因融合的关键信息,并且与免疫组织化学(IHC)一起,是进入研究性药物试验的患者临床决策中的宝贵工具。我们的目标是阐明晚期癌症患者原发部位与转移部位的突变谱,以指导合理治疗。所有晚期癌症的I期患者(n = 203)均通过市售的NGS平台进行分析。样本根据组织学、原发和转移部位、活检部位、基因突变、突变计数/基因以及突变体进行注释。每位患者的分子谱被分类为常见和独特突变、每个谱的信号通路以及映射到与DNA结合的p53三维结构和治疗前/后分子反应的突变。在分析的171例患者中,145例在原发和转移部位有基因改变。主要组织学类型为腺癌,其次是鳞状细胞癌、原发部位不明的癌(CUPS)和黑色素瘤。在790个独特突变中,KRAS是最常见的,其次是NRAS、BRAF、PIK3CA、AKT1、MAP2K1、MAP2K2、EGFR、NRAS、BRAF、PIK3CA、AKT1、MAP2K1、MAP2K2,且在大多数转移部位发现,似乎是获得性耐药的关键驱动因素。我们重点介绍了多种肿瘤类型在靶向治疗前/后获得性突变谱的例子以及一系列潜在的靶向药物。结论:癌症患者原发和转移病灶的突变谱分析为识别可能预测药物敏感性/耐药性并指导临床试验中合理药物组合的驱动“通路”提供了机会。