Department of Cardiology, Medical University of Vienna, Vienna, Austria.
Medical University of Vienna, IT Systems and Communications, Vienna, Austria.
Clin Res Cardiol. 2021 Jun;110(6):884-894. doi: 10.1007/s00392-021-01812-3. Epub 2021 Feb 10.
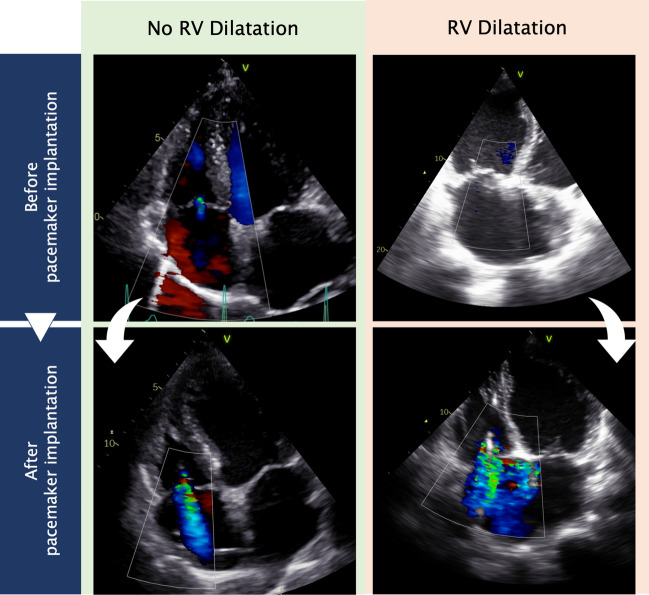
Transcatheter tricuspid valve intervention became an option for pacemaker lead-associated tricuspid regurgitation. This study investigated the progression of tricuspid regurgitation (TR) in patients with or without pre-existing right ventricular dilatation (RVD) undergoing pacemaker implantation.
Patients were included if they had implantation of transtricuspid pacemaker lead and completed echocardiography before and after implantation. The cohort was divided in patients with and without RVD (cut-off basal RV diameter ≥ 42 mm). TR was graded in none/mild, moderate, and severe. Worsening of one grade was defined as progression. Survival analyses were plotted for 10 years.
In total, 990 patients were analyzed (24.5% with RVD). Progression of TR occurred in 46.1% of patients with RVD and in 25.6% of patients without RVD (P < 0.001). Predictors for TR progression were RV dilatation (OR 2.04; 95% CI 1.27-3.29; P = 0.003), pre-existing TR (OR 4.30; 95% CI 2.51-7.38; P < 0.001), female sex (OR 1.68; 95% CI 1.16-2.43; P = 0.006), single RV lead (OR 1.67; 95% CI 1.09-2.56; P = 0.018), mitral regurgitation (OR 2.08; 95% CI 1.42-3.05; P < 0.001), and enlarged left atrium (OR 1.98; 95% CI 1.07-3.67; P = 0.03). Survival-predictors were pacemaker lead-associated TR (HR 1.38; 95% CI 1.04-1.84; P = 0.028), mitral regurgitation (HR 1.34; 95% CI 1.02-1.77; P = 0.034), heart failure (HR 1.75; 95% CI 1.31-2.33; P < 0.001), kidney disease (HR 1.62; 95% CI 1.25-2.11; P < 0.001), and age ≥ 80 years (HR 2.84; 95% CI 2.17-3.71; P < 0.001).
Patients with RVD receiving pacemaker suffered from increased TR progression, leading to decreased survival.
经导管三尖瓣介入治疗已成为与起搏器导线相关的三尖瓣反流的一种选择。本研究调查了在植入起搏器的患者中,有无预先存在的右心室扩张(RVD)的情况下三尖瓣反流(TR)的进展情况。
如果患者植入了经三尖瓣起搏器导线并在植入前后完成了超声心动图检查,则将其纳入研究。该队列分为有和无 RVD(基础 RV 直径≥42mm)的患者。TR 分为无/轻度、中度和重度。一个等级的恶化被定义为进展。绘制了 10 年的生存分析图。
共分析了 990 例患者(24.5%有 RVD)。有 RVD 的患者中有 46.1%发生 TR 进展,无 RVD 的患者中有 25.6%发生 TR 进展(P<0.001)。TR 进展的预测因素包括 RV 扩张(OR 2.04;95%CI 1.27-3.29;P=0.003)、预先存在的 TR(OR 4.30;95%CI 2.51-7.38;P<0.001)、女性(OR 1.68;95%CI 1.16-2.43;P=0.006)、单根 RV 导线(OR 1.67;95%CI 1.09-2.56;P=0.018)、二尖瓣反流(OR 2.08;95%CI 1.42-3.05;P<0.001)和左心房扩大(OR 1.98;95%CI 1.07-3.67;P=0.03)。生存预测因素包括起搏器导线相关的 TR(HR 1.38;95%CI 1.04-1.84;P=0.028)、二尖瓣反流(HR 1.34;95%CI 1.02-1.77;P=0.034)、心力衰竭(HR 1.75;95%CI 1.31-2.33;P<0.001)、肾脏疾病(HR 1.62;95%CI 1.25-2.11;P<0.001)和年龄≥80 岁(HR 2.84;95%CI 2.17-3.71;P<0.001)。
患有 RVD 的接受起搏器治疗的患者发生 TR 进展的风险增加,导致生存率降低。