Department of Mechanical Engineering, University of Canterbury, Christchurch, New Zealand.
Fisher and Paykel Healthcare, Auckland, New Zealand.
PLoS One. 2021 Feb 12;16(2):e0246123. doi: 10.1371/journal.pone.0246123. eCollection 2021.
Nasal High Flow (NHF) therapy delivers flows of heated humidified gases up to 60 LPM (litres per minute) via a nasal cannula. Particles of oral/nasal fluid released by patients undergoing NHF therapy may pose a cross-infection risk, which is a potential concern for treating COVID-19 patients.
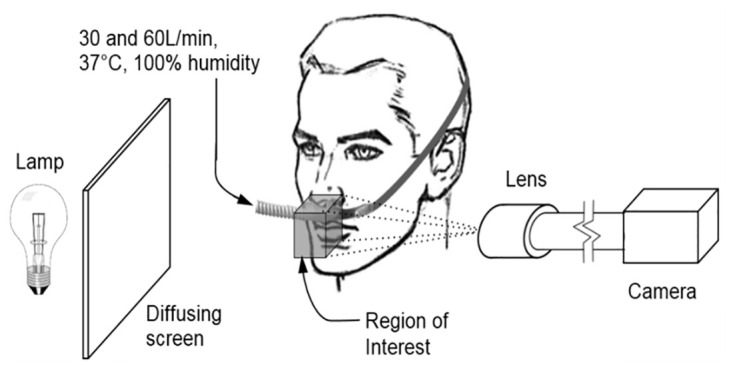
Liquid particles within the exhaled breath of healthy participants were measured with two protocols: (1) high speed camera imaging and counting exhaled particles under high magnification (6 participants) and (2) measuring the deposition of a chemical marker (riboflavin-5-monophosphate) at a distance of 100 and 500 mm on filter papers through which air was drawn (10 participants). The filter papers were assayed with HPLC. Breathing conditions tested included quiet (resting) breathing and vigorous breathing (which here means nasal snorting, voluntary coughing and voluntary sneezing). Unsupported (natural) breathing and NHF at 30 and 60 LPM were compared.
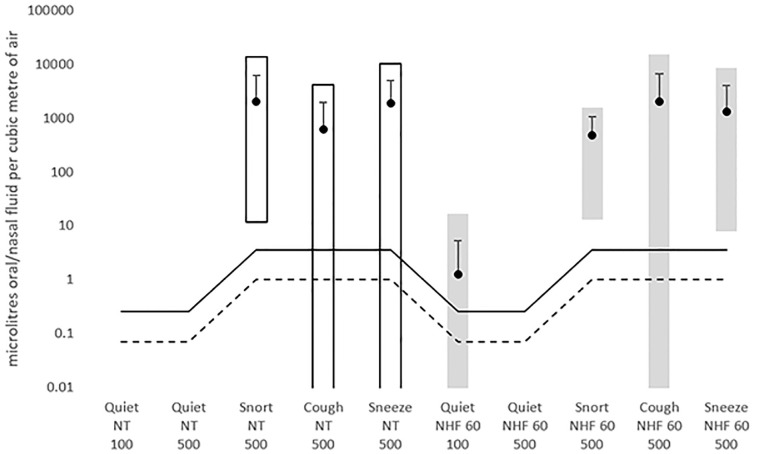
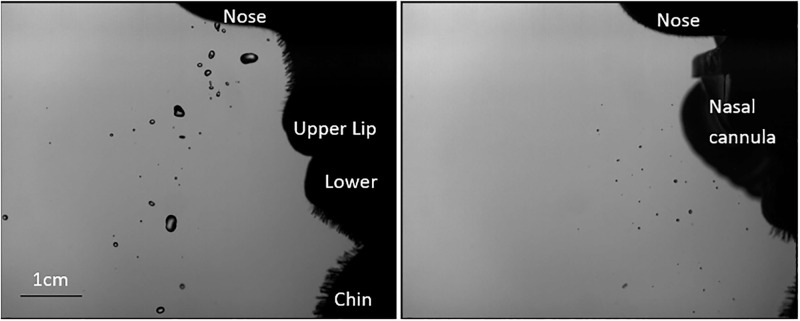
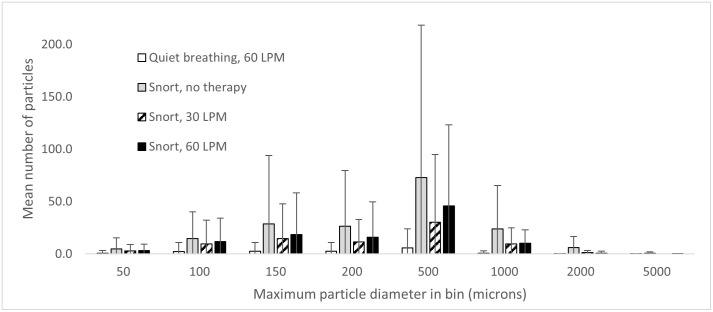
Imaging: During quiet breathing, no particles were recorded with unsupported breathing or 30 LPM NHF (detection limit for single particles 33 μm). Particles were detected from 2 of 6 participants at 60 LPM quiet breathing at approximately 10% of the rate caused by unsupported vigorous breathing. Unsupported vigorous breathing released the greatest numbers of particles. Vigorous breathing with NHF at 60 LPM, released half the number of particles compared to vigorous breathing without NHF.Chemical marker tests: No oral/nasal fluid was detected in quiet breathing without NHF (detection limit 0.28 μL/m3). In quiet breathing with NHF at 60 LPM, small quantities were detected in 4 out of 29 quiet breathing tests, not exceeding 17 μL/m3. Vigorous breathing released 200-1000 times more fluid than the quiet breathing with NHF. The quantities detected in vigorous breathing were similar whether using NHF or not.
During quiet breathing, 60 LPM NHF therapy may cause oral/nasal fluid to be released as particles, at levels of tens of μL per cubic metre of air. Vigorous breathing (snort, cough or sneeze) releases 200 to 1000 times more oral/nasal fluid than quiet breathing (p < 0.001 with both imaging and chemical marker methods). During vigorous breathing, 60 LPM NHF therapy caused no statistically significant difference in the quantity of oral/nasal fluid released compared to unsupported breathing. NHF use does not increase the risk of dispersing infectious aerosols above the risk of unsupported vigorous breathing. Standard infection prevention and control measures should apply when dealing with a patient who has an acute respiratory infection, independent of which, if any, respiratory support is being used.
ACTRN12614000924651.
鼻高流量(NHF)治疗通过鼻插管输送加热加湿的气体,流速可达 60 升/分钟(升/分钟)。接受 NHF 治疗的患者释放的口腔/鼻腔液体颗粒可能会带来交叉感染的风险,这是治疗 COVID-19 患者的一个潜在问题。
使用两种方案测量健康参与者呼出的液体颗粒:(1)高速摄像成像并在高倍放大下计数呼出的颗粒(6 名参与者)和(2)通过在距滤纸 100 和 500 毫米处测量化学标记物(核黄素-5-单磷酸盐)的沉积量,空气通过滤纸(10 名参与者)。滤纸用 HPLC 进行分析。测试的呼吸条件包括安静(休息)呼吸和剧烈呼吸(这里指的是鼻吸气、自愿咳嗽和自愿打喷嚏)。比较了无支撑(自然)呼吸和 30 和 60 升/分钟的 NHF。
成像:在安静呼吸期间,未记录到无支撑呼吸或 30 升/分钟 NHF 时的颗粒(单个颗粒的检测限为 33 μm)。在 6 名参与者中的 2 名参与者以大约 10%的速度在 60 升/分钟的安静呼吸中检测到颗粒,而不受支持的剧烈呼吸速度更快。无支撑剧烈呼吸释放的颗粒数量最多。与无 NHF 的剧烈呼吸相比,60 升/分钟 NHF 下的剧烈呼吸释放的颗粒数量减少了一半。
无 NHF 的安静呼吸中未检测到口腔/鼻腔液体(检测限 0.28 μL/m3)。在 60 升/分钟 NHF 的安静呼吸中,在 29 次安静呼吸测试中的 4 次中检测到少量(不超过 17 μL/m3)。剧烈呼吸释放的液体量是安静呼吸时使用 NHF 的 200-1000 倍。使用 NHF 或不使用 NHF 时,剧烈呼吸释放的液体量相似。
在安静呼吸期间,60 升/分钟的 NHF 治疗可能会导致口腔/鼻腔液体以数十微升/立方米空气的水平作为颗粒释放。剧烈呼吸(鼻吸气、咳嗽或打喷嚏)释放的口腔/鼻腔液体量比安静呼吸多 200 到 1000 倍(两种成像和化学标记方法均 p < 0.001)。在剧烈呼吸时,与无支撑呼吸相比,60 升/分钟 NHF 治疗对释放的口腔/鼻腔液体量没有统计学上的显著差异。与无支撑剧烈呼吸相比,使用 NHF 不会增加传染性气溶胶分散的风险。在处理患有急性呼吸道感染的患者时,应采用标准的感染预防和控制措施,无论患者正在使用哪种呼吸支持,无论使用何种呼吸支持。
ACTRN12614000924651。