Department of Cardiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, No. 1, DaHua Road, Dong Dan, Beijing, 100730, P. R. China.
BMC Geriatr. 2021 Feb 16;21(1):125. doi: 10.1186/s12877-021-02072-6.
Frailty increases the adverse outcomes of clinical heart failure; however, the relationship between frailty and stage-B heart failure (SBHF) remains unknown. We aimed to explore the epidemiology and predictive value of frailty in older adults with SBHF.
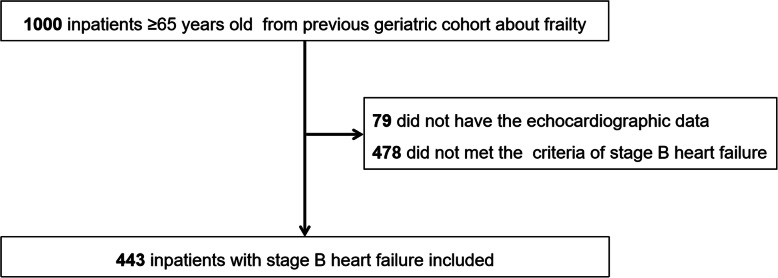
A prospective cohort of SBHF inpatients aged 65 years or older who were hospitalized between September 2018 and February 2019 and were followed up for 6 months were included. SBHF was defined as systolic abnormality, structural abnormality (left ventricular enlargement, left ventricular hypertrophy, wall motion abnormalities, valvular heart disease), or prior myocardial infarction. Frailty was assessed by the Fried frailty phenotype. Multivariable Cox proportional hazards regression was used to explore the independent risk and prognostic factors.
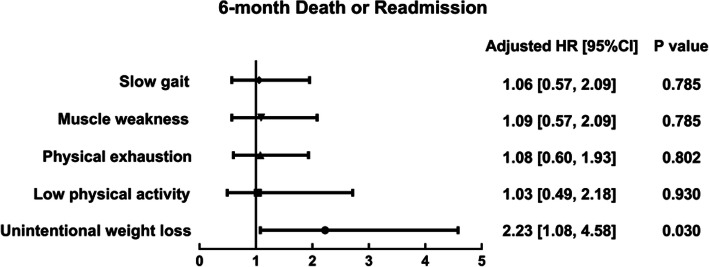
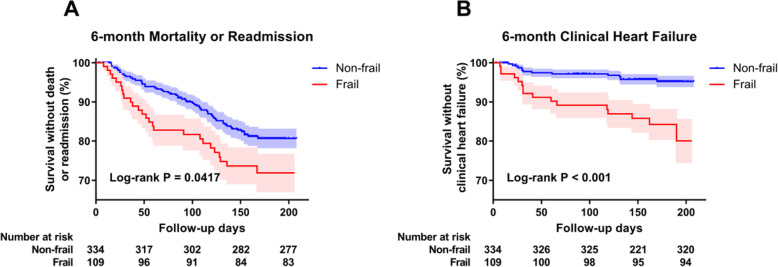
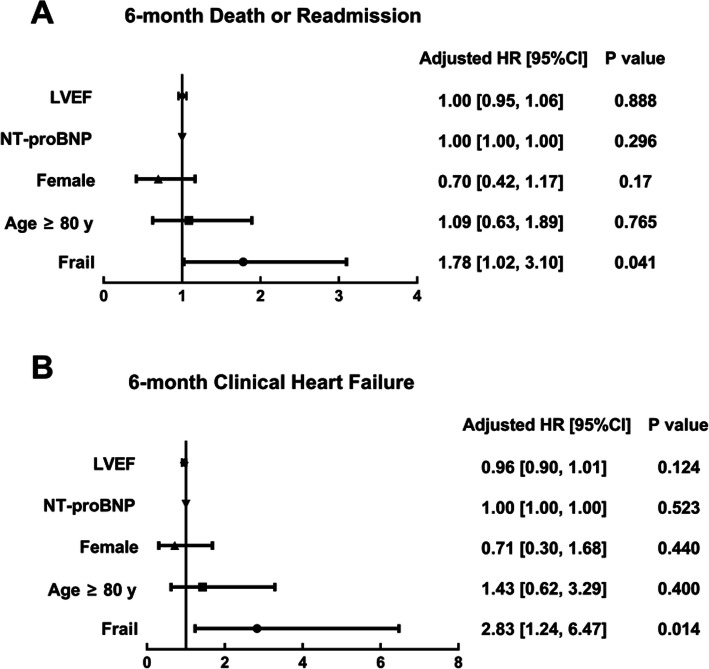
Data of 443 participants (age: 76.1 ± 6.79 years, LVEF: 62.8 ± 4.92%, men: 225 [50.8%], frailty: 109 [24.6%]) were analyzed. During the 6-month follow-up, 83 (18.7%) older SBHF inpatients experienced all-cause mortality or readmission, and 29 (6.5%) of them developed clinical HF. Frail individuals had a 1.78-fold (95%CI: 1.02-3.10, P = 0.041) higher risk of 6-month mortality or readmission and a 2.83-fold (95%CI 1.24-6.47, P = 0.014) higher risk of developing clinical HF, independent of age, sex, left ventricular ejection fraction, and N-terminal pro-B-type natriuretic peptide level.
Frailty is common in older SBHF inpatients and should be considered to help identify individuals with an increased risk of mortality or readmission, and developing clinical HF.
ChiCTR1800017204 .
衰弱会增加临床心力衰竭的不良后果;然而,衰弱与 B 期心力衰竭(SBHF)之间的关系尚不清楚。我们旨在探讨老年 SBHF 患者衰弱的流行病学和预测价值。
纳入 2018 年 9 月至 2019 年 2 月期间住院的年龄在 65 岁或以上的 SBHF 住院患者进行前瞻性队列研究,并随访 6 个月。SBHF 定义为收缩功能异常、结构异常(左心室扩大、左心室肥厚、室壁运动异常、瓣膜性心脏病)或既往心肌梗死。衰弱通过 Fried 衰弱表型进行评估。多变量 Cox 比例风险回归用于探讨独立的风险和预后因素。
共分析了 443 名参与者(年龄:76.1±6.79 岁,LVEF:62.8±4.92%,男性:225[50.8%],衰弱:109[24.6%])的数据。在 6 个月的随访期间,83 名(18.7%)老年 SBHF 住院患者经历了全因死亡率或再入院,其中 29 名(6.5%)发生了临床 HF。衰弱患者 6 个月死亡率或再入院的风险增加 1.78 倍(95%CI:1.02-3.10,P=0.041),发生临床 HF 的风险增加 2.83 倍(95%CI 1.24-6.47,P=0.014),独立于年龄、性别、左心室射血分数和 N 末端 pro-B 型利钠肽水平。
衰弱在老年 SBHF 住院患者中很常见,应考虑用于识别死亡率或再入院风险增加以及发生临床 HF 的个体。
ChiCTR1800017204。