Swedish Health Services, 600 Broadway, Suite 610, Seattle, WA, 98122, USA.
School of Public Health, University of Washington, Seattle, WA, USA.
Crit Care. 2021 Feb 17;25(1):70. doi: 10.1186/s13054-021-03504-w.
The early months of the COVID-19 pandemic were fraught with much uncertainty and some resource constraint. We assessed the change in survival to hospital discharge over time for intensive care unit patients with COVID-19 during the first 3 months of the pandemic and the presence of any surge effects on patient outcomes.
Retrospective cohort study using electronic medical record data for all patients with laboratory-confirmed COVID-19 admitted to intensive care units from February 25, 2020, to May 15, 2020, at one of 26 hospitals within an integrated delivery system in the Western USA. Patient demographics, comorbidities, and severity of illness were measured along with medical therapies and hospital outcomes over time. Multivariable logistic regression models were constructed to assess temporal changes in survival to hospital discharge during the study period.
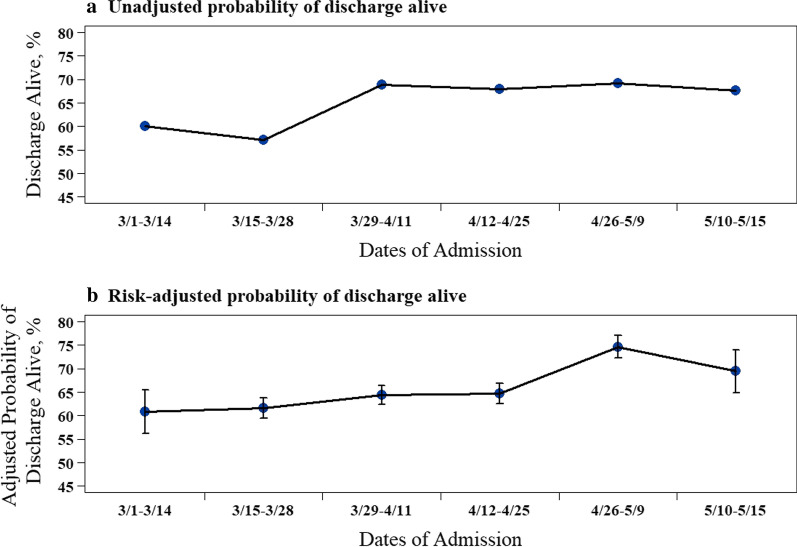
Of 620 patients with COVID-19 admitted to the ICU [mean age 63.5 years (SD 15.7) and 69% male], 403 (65%) survived to hospital discharge and 217 (35%) died in the hospital. Survival to hospital discharge increased over time, from 60.0% in the first 2 weeks of the study period to 67.6% in the last 2 weeks. In a multivariable logistic regression analysis, the risk-adjusted odds of survival to hospital discharge increased over time (biweekly change, adjusted odds ratio [aOR] 1.22, 95% CI 1.04-1.40, P = 0.02). Additionally, an a priori-defined explanatory model showed that after adjusting for both hospital occupancy and percent hospital capacity by COVID-19-positive individuals and persons under investigation (PUI), the temporal trend in risk-adjusted patient survival to hospital discharge remained the same (biweekly change, aOR 1.18, 95% CI 1.00-1.38, P = 0.04). The presence of greater rates of COVID-19 positive/PUI as a percentage of hospital capacity was, however, significantly and inversely associated with survival to hospital discharge (aOR 0.95, 95% CI 0.92-0.98, P < 0.01).
During the early COVID-19 pandemic, risk-adjusted survival to hospital discharge increased over time for critical care patients. An association was also seen between a greater COVID-19-positive/PUI percentage of hospital capacity and a lower survival rate to hospital discharge.
在 COVID-19 大流行的早期,存在着许多不确定性和一些资源限制。我们评估了在大流行的头 3 个月期间,重症监护病房中 COVID-19 患者的住院存活率随时间的变化,以及对患者预后是否存在任何激增效应。
这是一项回顾性队列研究,使用了美国西部 26 家医院综合医疗系统内 2 月 25 日至 5 月 15 日期间,所有经实验室确诊的 COVID-19 入住重症监护病房的患者的电子病历数据。患者的人口统计学、合并症和疾病严重程度以及随时间推移的医疗治疗和医院结局都进行了测量。采用多变量逻辑回归模型评估研究期间住院存活率随时间的变化。
620 例 COVID-19 重症监护病房患者中,403 例(65%)存活至出院,217 例(35%)在医院死亡。随着时间的推移,住院存活率逐渐升高,从研究开始的前 2 周的 60.0%升高至最后 2 周的 67.6%。在多变量逻辑回归分析中,调整后的存活至出院的风险比随着时间的推移而增加(每两周变化,调整后的优势比[aOR]1.22,95%置信区间[CI]1.04-1.40,P=0.02)。此外,一个预先定义的解释模型表明,在调整了医院入住率和 COVID-19 阳性患者及待调查者(Person Under Investigation,PUI)所占医院容量的百分比后,风险调整后患者住院存活率的时间趋势仍然相同(每两周变化,aOR 1.18,95%CI 1.00-1.38,P=0.04)。然而,COVID-19 阳性/PUI 占医院容量的百分比越高,与出院存活率呈显著负相关(aOR 0.95,95%CI 0.92-0.98,P<0.01)。
在 COVID-19 大流行的早期,重症监护患者的风险调整后住院存活率随时间逐渐增加。此外,COVID-19 阳性/PUI 患者占医院容量的百分比与出院存活率呈负相关。