Centre for Heart Lung Innovation, St Pauls Hospital, The University of British Columbia, Vancouver, BC, Canada.
Research Institute McGill University Health Centre, McGill University, Montreal, Quebec, Canada.
Int J Chron Obstruct Pulmon Dis. 2021 Feb 12;16:305-320. doi: 10.2147/COPD.S285338. eCollection 2021.
To determine the spirometric-based prevalence of COPD across different regions in Canada and to evaluate the site heterogeneity of risk factors.
In this cross-sectional, population-based study, random samples of non-institutionalized adults aged ≥40 years were generated by random digit dialling. Participants answered an interviewer-administered questionnaire and performed spirometry before and after bronchodilator administration. COPD was defined as post-bronchodilator FEV/FVC <0.70 (fixed ratio, FR) and as FEV/FVC <5th percentile (lower limits of normal, LLN). Separate logistic regression models were used to compute the risk (adjusted odds ratio, aOR) for COPD. I and Tau analyses were used to evaluate heterogeneity.
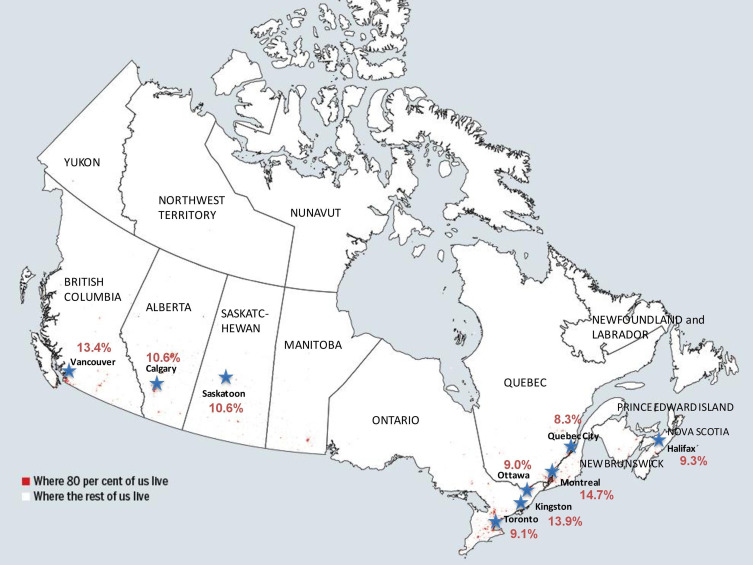
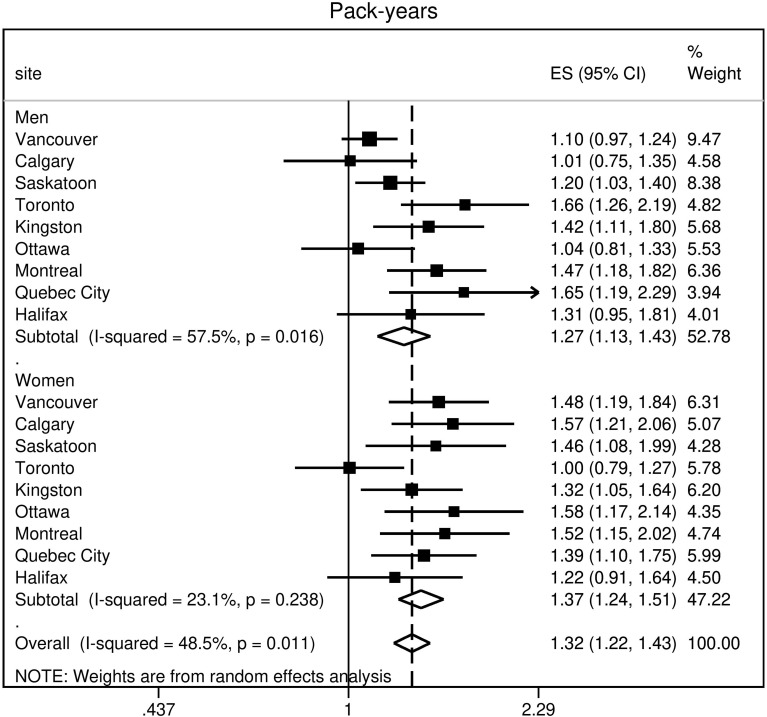
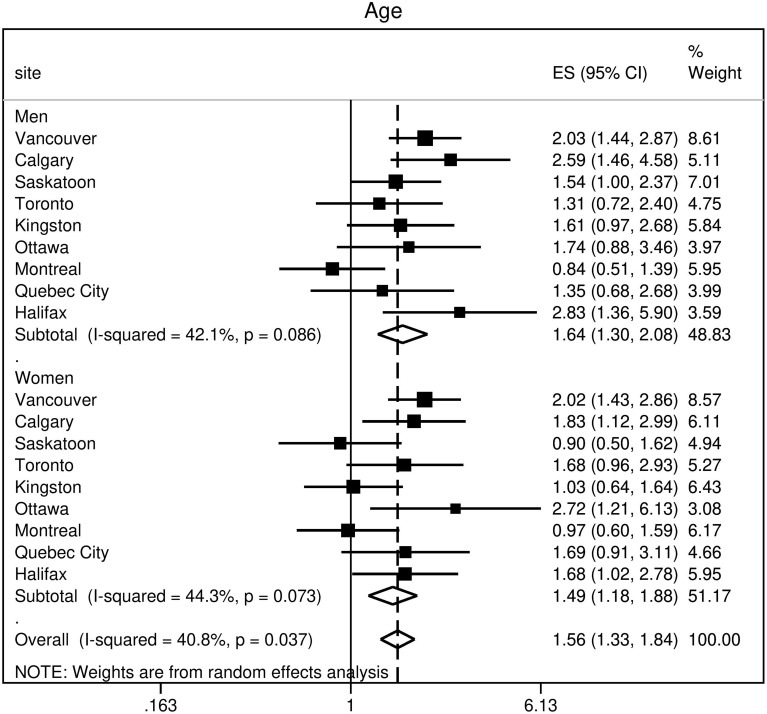
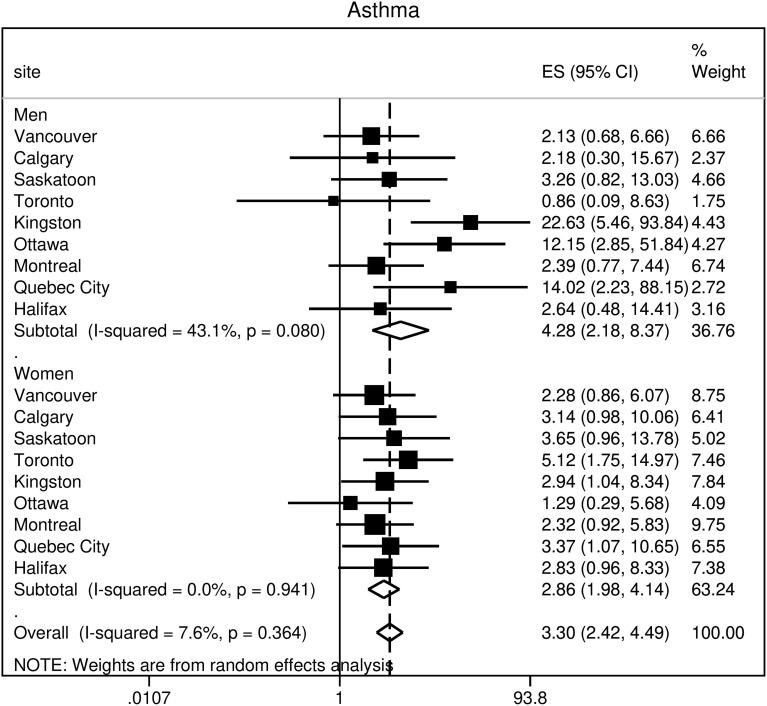
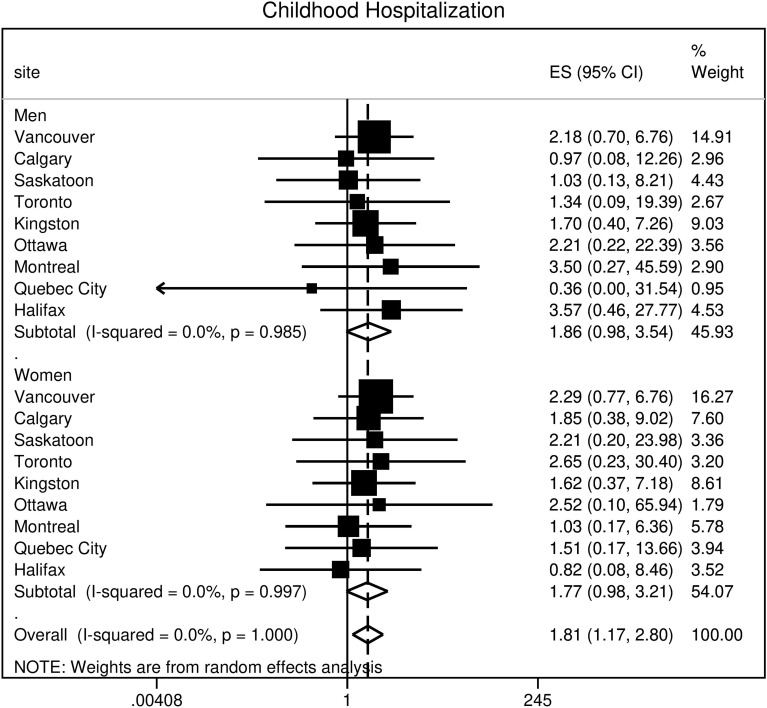
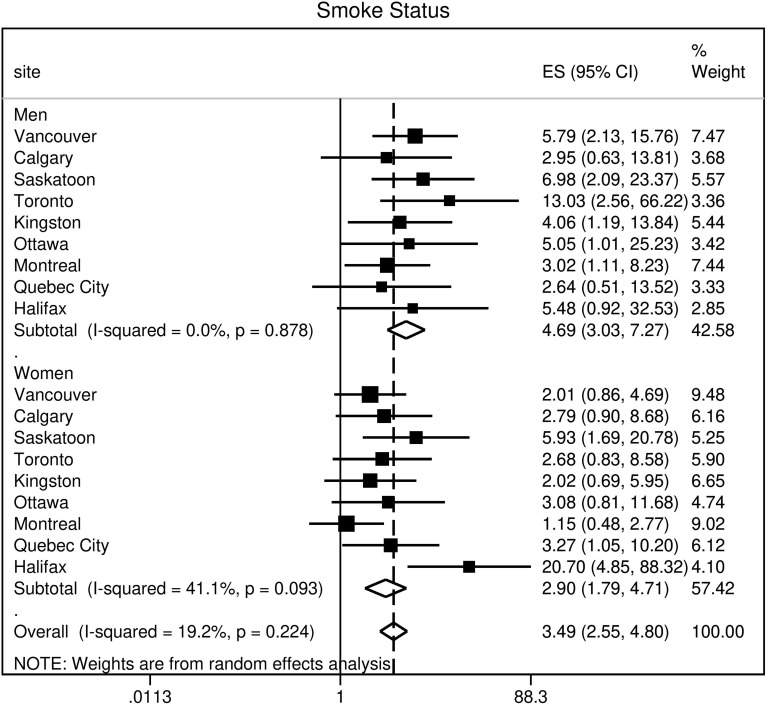
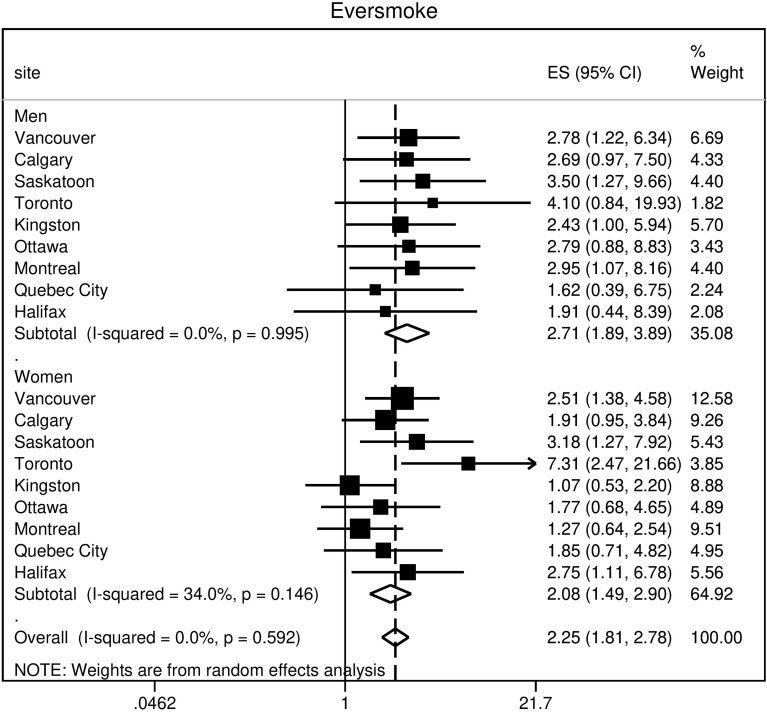
Out of 5176 (95%) participants, 4893 (47% male with mean age 56.6 years (95% confidence interval, 56.0-57.2)) had spirometry that satisfied ATS criteria. The population prevalence of COPD was 16.2% (95% CI, 14.5-17.8) by FR and 11.2% (95% CI, 9.7-12.6) by LLN. Male predominance in prevalence was shown by FR but not by LLN criteria. Patient characteristics associated with an increased risk of COPD included: age (OR 1.56; 95% CI 1.33-1.84); history of physician-diagnosed asthma (OR 3.30; 95% CI 2.42-4.49); and childhood hospitalization for respiratory illness (OR 1.81; 95% CI 1.17-2.80). In terms of smoking-related risk factors, current smoking status had the highest odds ratio (OR 3.49; 95% CI 2.55-4.80). Variance in prevalence among sites was significantly reduced by adjusting for risk factors in Tau analyses. Higher odds of exposure for each risk factor was found in more severe COPD, suggesting that a higher risk could be linked to the development of severe disease.
This study reports the population prevalence of COPD in nine urban cities which collectively represent the majority of the Canadian population and demonstrates that heterogeneity in prevalence among sites is substantially explained by variation in associated risk factors for COPD.
确定加拿大不同地区基于肺量计的 COPD 患病率,并评估危险因素的部位异质性。
在这项横断面、基于人群的研究中,通过随机数字拨号生成非机构化成年人群的随机样本,年龄≥40 岁。参与者回答了一个由调查员管理的问卷,并在支气管扩张剂给药前后进行了肺量计检查。COPD 定义为支气管扩张剂后 FEV/FVC<0.70(固定比值,FR)和 FEV/FVC<5 百分位数(正常下限,LLN)。分别使用逻辑回归模型计算 COPD 的风险(调整后的优势比,aOR)。使用 I ²和 Tau 分析评估异质性。
在 5176 名(95%)参与者中,4893 名(47%为男性,平均年龄 56.6 岁(95%置信区间,56.0-57.2))的肺量计符合 ATS 标准。根据 FR,COPD 的人群患病率为 16.2%(95%CI,14.5-17.8),根据 LLN 为 11.2%(95%CI,9.7-12.6)。FR 显示男性患病率较高,但 LLN 标准则不然。与 COPD 风险增加相关的患者特征包括:年龄(OR 1.56;95%CI 1.33-1.84);医生诊断的哮喘病史(OR 3.30;95%CI 2.42-4.49);和儿童时期因呼吸道疾病住院(OR 1.81;95%CI 1.17-2.80)。就与吸烟相关的危险因素而言,当前吸烟状况的比值比最高(OR 3.49;95%CI 2.55-4.80)。在 Tau 分析中,通过调整 COPD 相关危险因素,站点间患病率的方差显著降低。对于每个危险因素,较高的暴露几率与更严重的 COPD 相关,这表明更高的风险可能与严重疾病的发展有关。
本研究报告了加拿大九个城市的 COPD 人群患病率,这些城市共同代表了加拿大的大部分人口,并表明站点间患病率的异质性在很大程度上可以通过 COPD 相关危险因素的差异来解释。