Beydoun Sarah A, Iorio Olivia C, Genkin Daniel, Li Pei Z, Doiron Dany, Maltais François, Bourbeau Jean, Tan Wan, Sin Don D, Aaron Shawn D, Chapman Kenneth R, Hernandez Paul, Marciniuk Darcy D, O'Donnell Denis E, Walker Brandie L, Kirby Miranda, Ross Bryan A
Respiratory Epidemiology and Clinical Research Unit, Centre for Outcomes Research and Evaluation, Research Institute of the McGill University Health Centre, Montreal, QC, Canada.
Department of Medicine, Faculty of Medicine and Health Sciences, McGill University, Montreal, Canada.
ERJ Open Res. 2025 Jun 30;11(3). doi: 10.1183/23120541.01042-2024. eCollection 2025 May.
Dynamic hyperinflation is central to dyspnoea, exercise limitation and exacerbations in COPD. While studied previously in moderate-to-severe COPD, the relevance of diaphragm dome height (DDH) on clinically important outcomes has been under-investigated in mild-to-moderate COPD.
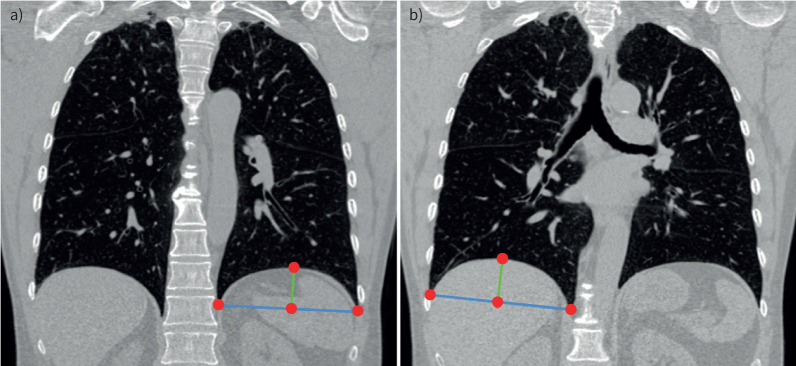
Canadian Cohort Obstructive Lung Disease (CanCOLD) participants with spirometry-confirmed COPD, symptom-limited incremental cardiopulmonary exercise testing and computed tomography image data were included. Base-to-apex left DDH (LDDH) and right DDH (RDDH) were automatically segmented, with increased height implying less flattening and thus less hyperinflation. Dynamic hyperinflation was defined as ≥150 mL reduction in inspiratory capacity (IC) from rest to peak exercise. Cross-sectional linear regression models were fitted between LDDH and RDDH (predictor variables) with peak IC (IC), peak workload ( ), forced expiratory volume in 1 s (FEV) and COPD Assessment Test (CAT) score (outcome variables), and in longitudinal (Anderson-Gill) models with "symptom-based" and "event-based" exacerbations. Results are reported as parameter estimates or hazard ratios (HRs) with 95% confidence intervals per interquartile range dome height increment.
Amongst 304 participants (mean±sd age 64.7±10.3 years, 41.8% female, 44.4% with mild COPD), each LDDH and RDDH increment, respectively, was associated with IC (0.21 (95% CI 0.13-0.29) L and 0.13 (95% CI 0.07-0.19) L), (9.54 (95% CI 5.03-14.04) W and 6.04 (95% CI 2.45-9.62) W), FEV (0.17 (95% CI 0.10-0.25) L and 0.08 (95% CI 0.02-0.14) L) and CAT score (-1.36 (95% CI -2.39- -0.33) and -0.82 (95% CI -1.63-0.00)). LDDH alone was associated with both symptom-based (HR 0.82 (95% CI 0.74-0.91)) and event-based (HR 0.83 (95% CI 0.73-0.95)) exacerbations. Of 167 out of 304 participants with confirmed dynamic hyperinflation (ΔIC -0.47±0.25 L), LDDH alone was associated with all outcomes (IC, , FEV, CAT and symptom-based/event-based exacerbations).
LDDH appears to be a clinically important marker for operational lung volume changes, lung function, exercise performance, disease burden and exacerbations in mild-to-moderate COPD.
动态肺过度充气是慢性阻塞性肺疾病(COPD)患者呼吸困难、运动受限和病情加重的核心问题。虽然此前已在中重度COPD中进行过研究,但在轻度至中度COPD中,膈肌穹窿高度(DDH)对临床重要结局的相关性研究不足。
纳入加拿大队列阻塞性肺病(CanCOLD)研究中肺活量测定确诊为COPD的参与者,进行症状限制递增式心肺运动试验及计算机断层扫描图像数据采集。自动分割左膈肌穹窿高度(LDDH)和右膈肌穹窿高度(RDDH),高度增加意味着扁平化程度降低,即肺过度充气程度降低。动态肺过度充气定义为吸气容量(IC)从静息状态到运动峰值时减少≥150 mL。在LDDH和RDDH(预测变量)与峰值IC(IC)、峰值工作量( )、第1秒用力呼气量(FEV)和COPD评估测试(CAT)评分(结局变量)之间建立横断面线性回归模型,并在纵向(Anderson-Gill)模型中分析与“基于症状”和“基于事件”的病情加重情况的关系。结果以每四分位数间距穹窿高度增加的参数估计值或风险比(HRs)及95%置信区间报告。
在304名参与者中(平均±标准差年龄64.7±10.3岁,41.8%为女性,44.4%为轻度COPD),LDDH和RDDH每增加一个单位,分别与IC增加(0.21(95%CI 0.13 - 0.29)L和0.13(95%CI 0.07 - 0.19)L)、 增加(9.54(95%CI 5.03 - 14.04)W和6.04(95%CI 2.45 - 9.62)W)、FEV增加(0.17(95%CI 0.10 - 0.25)L和0.08(95%CI 0.开1.63 - 0.00))和CAT评分降低(-1.36(95%CI -2.39 - -0.33)和-0.82(95%CI -1.63 - 开0.00))相关。仅LDDH与基于症状的病情加重(HR 0.82(95%CI 0.74 - 0.91))和基于事件的病情加重(HR 0.83(95%CI 0.73 - 0.95))均相关。在304名确诊为动态肺过度充气(ΔIC -0.47±0.25 L)的参与者中,有167名,仅LDDH与所有结局(IC、 、FEV、CAT及基于症状/基于事件的病情加重)相关。
LDDH似乎是轻度至中度COPD患者肺容积变化、肺功能、运动表现、疾病负担和病情加重的重要临床标志物。