Department of Neurosurgery, Spine Center, Gachon University Gil Medical Center, Gachon University College of Medicine, Incheon, Korea.
Department of Neurosurgery, Spine Center, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
J Korean Med Sci. 2021 Feb 22;36(7):e52. doi: 10.3346/jkms.2021.36.e52.
Surgery for spinal metastasis is rapidly increasing in frequency with procedures ranging from laminectomy to spondylectomy combined with stabilization. This study investigated the effect of various surgical procedures for spinal metastasis of non-small cell lung cancer (NSCLC).
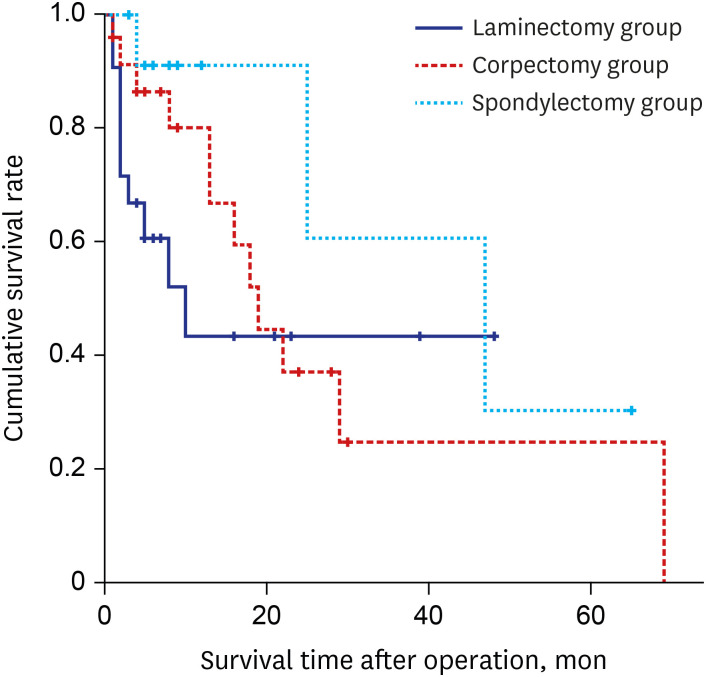
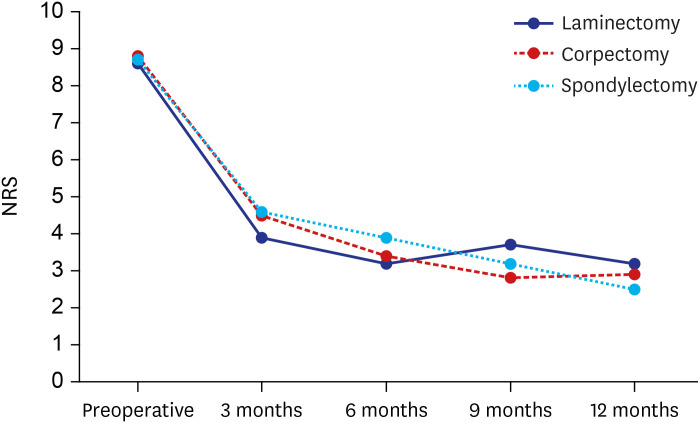
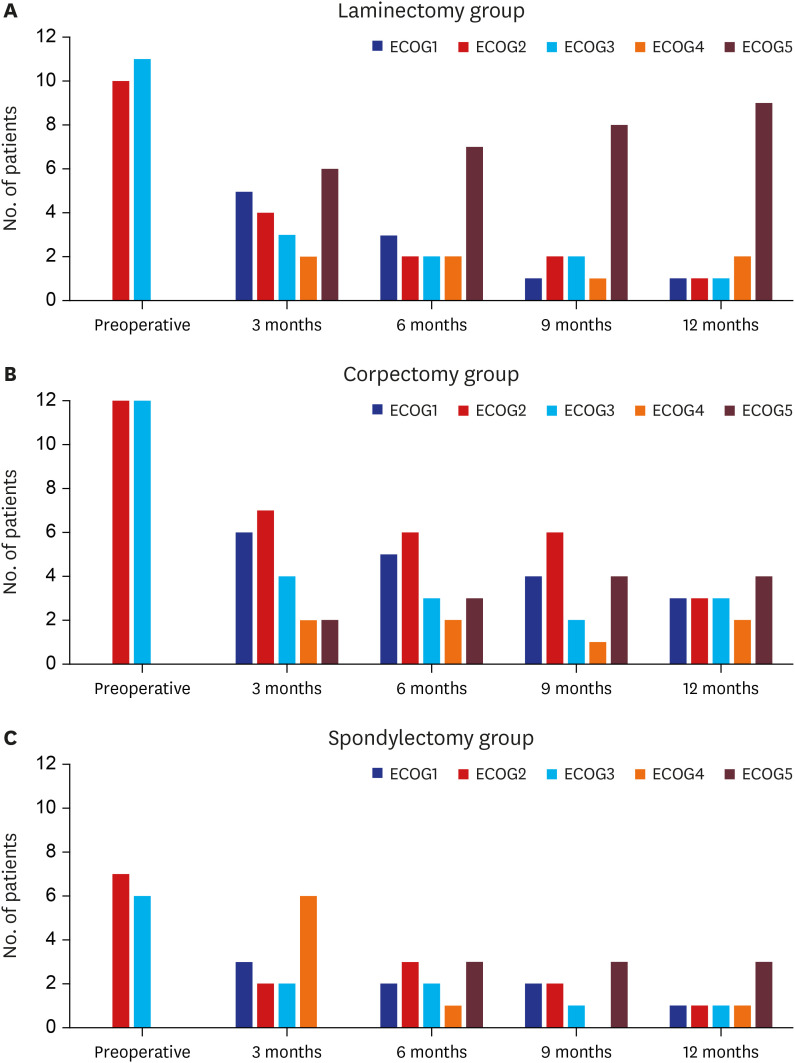
A single-center consecutive series of patients who underwent surgery for spinal metastasis of NSCLC were retrospectively reviewed. Patients' characteristics, radiographic parameters, operative data, clinical outcomes, and complications were analyzed. Surgical outcomes were assessed according to pain and performance status before and after surgery. Overall survival (OS) rate was estimated using the Kaplan-Meier method. Multivariate analysis was performed to detect factors independently associated with OS using a Cox proportional hazards model.
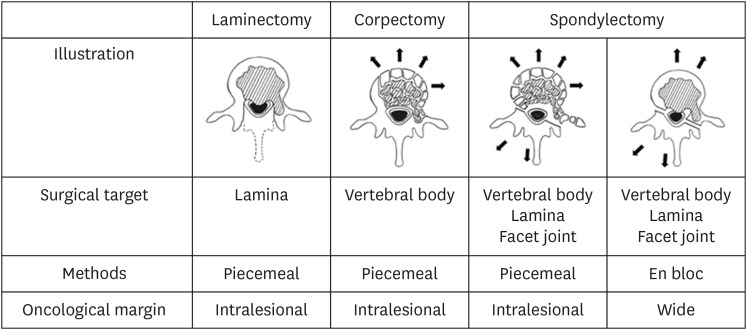
Twenty-one patients were treated with laminectomy, 24 with corpectomy, 13 with spondylectomy (piecemeal or total en bloc fashion), and all procedures were combined with stabilization. Back pain and performance status improved significantly after surgical treatment among the three groups. Revision surgery due to tumor progression at the index level or spinal metastasis at another level were four patients (19.0%) in the laminectomy group, six patients (25.0%) in the corpectomy group, and one patient (7.7%) in the spondylectomy group. A Charlson comorbidity index and the number of spinal metastasis negatively affected OS (hazard ratio [HR], 19.613 and 2.244). Postoperative chemotherapy, time to metastasis, spondylectomy, and corpectomy had favorable associations with OS (HR, 0.455, 0.487, 0.619, and 0.715, respectively).
Postoperative chemotherapy was the most critical factor in OS of patients with metastatic NSCLC to the spine. An extensive surgical procedure (corpectomy/spondylectomy) with stabilization also could be beneficial for limited patients with spinal metastasis of NSCLC.
脊柱转移瘤的手术治疗频率迅速增加,手术范围从椎板切除术到椎体切除术联合稳定术。本研究调查了各种手术方法治疗非小细胞肺癌(NSCLC)脊柱转移的效果。
回顾性分析了在我院接受 NSCLC 脊柱转移手术的患者的临床资料。分析患者的一般特征、影像学参数、手术数据、临床结局和并发症。根据手术前后的疼痛和功能状态评估手术结果。使用 Kaplan-Meier 方法估计总生存率(OS)。使用 Cox 比例风险模型进行多变量分析,以确定与 OS 独立相关的因素。
21 例患者接受了椎板切除术,24 例患者接受了椎体切除术,13 例患者接受了椎体切除术(部分或整块),所有手术均结合了稳定术。三组患者的腰痛和功能状态在手术后均显著改善。在索引水平肿瘤进展或其他水平脊柱转移导致需要翻修手术的患者中,椎板切除术组有 4 例(19.0%),椎体切除术组有 6 例(25.0%),椎体切除术组有 1 例(7.7%)。Charlson 合并症指数和脊柱转移数量对 OS 有负面影响(风险比 [HR] 为 19.613 和 2.244)。术后化疗、转移时间、椎体切除术和椎体切除术与 OS 有良好的相关性(HR 分别为 0.455、0.487、0.619 和 0.715)。
术后化疗是影响 NSCLC 脊柱转移患者 OS 的最重要因素。广泛的手术(椎体切除术/椎体切除术)联合稳定术也可能对有限的 NSCLC 脊柱转移患者有益。