Institute for Diagnostic and Interventional Radiology, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany.
Department of Radiology, University Hospitals Cleveland Medical Center, Cleveland, OH, USA.
Eur Radiol. 2021 Sep;31(9):7151-7161. doi: 10.1007/s00330-021-07746-8. Epub 2021 Feb 25.
To evaluate the reduction of artifacts from cardiac implantable electronic devices (CIEDs) by virtual monoenergetic images (VMI), metal artifact reduction (MAR) algorithms, and their combination (VMI) derived from spectral detector CT (SDCT) of the chest compared to conventional CT images (CI).
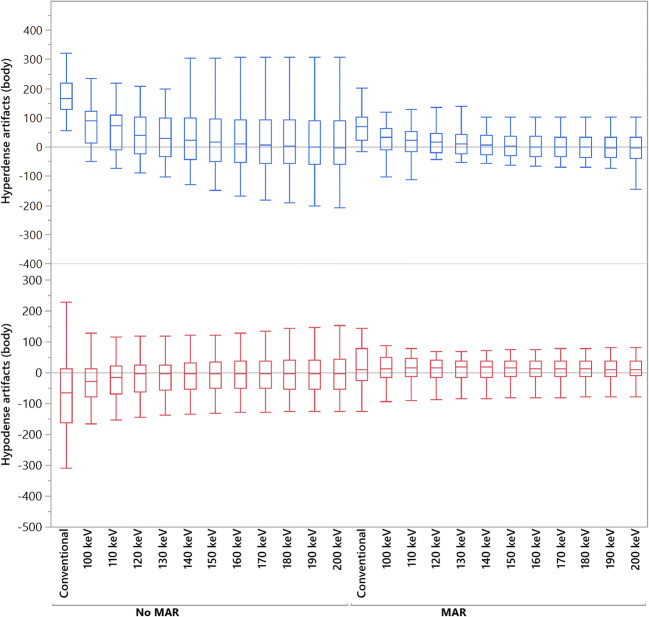
In this retrospective study, we included 34 patients (mean age 74.6 ± 8.6 years), who underwent a SDCT of the chest and had a CIED in place. CI, MAR, VMI, and VMI (10 keV increment, range: 100-200 keV) were reconstructed. Mean and standard deviation of attenuation (HU) among hypo- and hyperdense artifacts adjacent to CIED generator and leads were determined using ROIs. Two radiologists qualitatively evaluated artifact reduction and diagnostic assessment of adjacent tissue.
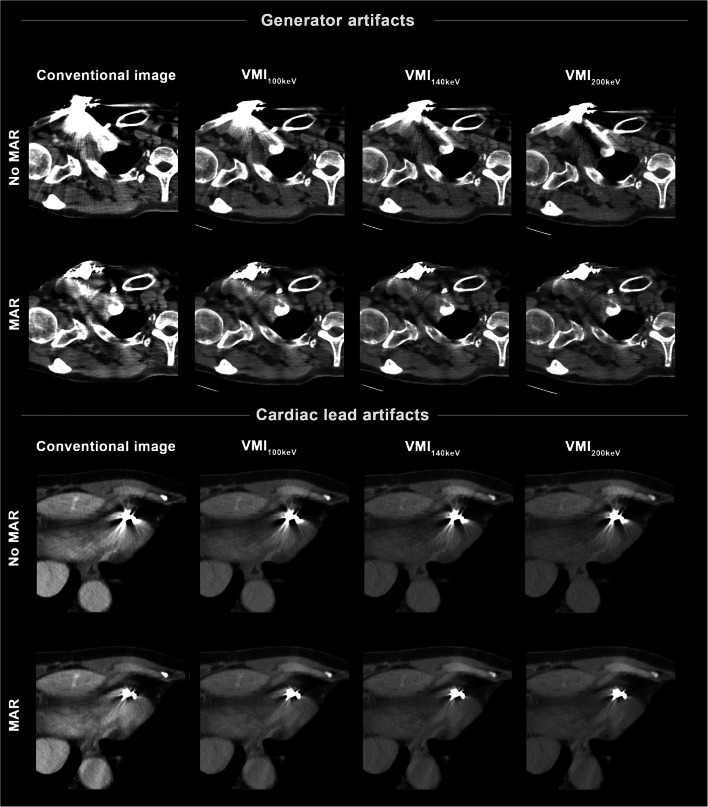
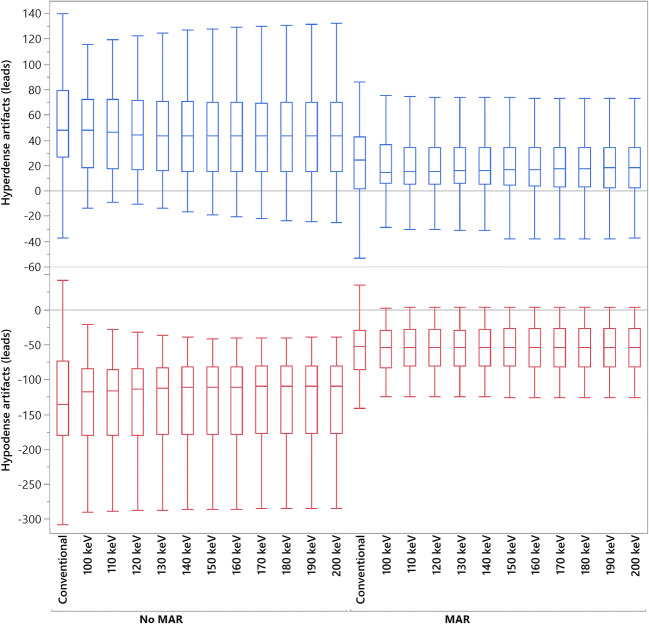
Compared to CI, MAR and VMI ≥ 100 keV significantly increased attenuation in hypodense and significantly decreased attenuation in hyperdense artifacts at CIED generator and leads (p < 0.05). VMI ≥ 100 keV alone only significantly decreased hyperdense artifacts at the generator (p < 0.05). Qualitatively, VMI ≥ 100 keV, MAR, and VMI ≥ 100 keV provided significant reduction of hyper- and hypodense artifacts resulting from the generator and improved diagnostic assessment of surrounding structures (p < 0.05). Diagnostic assessment of structures adjoining to the leads was only improved by MAR and VMI 100 keV (p < 0.05), whereas keV values ≥ 140 with and without MAR significantly worsened diagnostic assessment (p < 0.05).
The combination of VMI and MAR as well as MAR as a standalone approach provides effective reduction of artifacts from CIEDs. Still, higher keV values should be applied with caution due to a loss of soft tissue and vessel contrast along the leads.
• The combination of VMI and MAR as well as MAR as a standalone approach enables effective reduction of artifacts from CIEDs. • Higher keV values of both VMI and VMI at CIED leads should be applied with caution since diagnostic assessment can be hampered by a loss of soft tissue and vessel contrast. • Recommended keV values for CIED generators are between 140 and 200 keV and for leads around 100 keV.
评估与常规 CT 图像(CI)相比,胸部光谱探测器 CT(SDCT)的虚拟单能量图像(VMI)、金属伪影减少(MAR)算法及其组合(VMI)在减少心脏植入式电子设备(CIED)伪影方面的效果。
在这项回顾性研究中,我们纳入了 34 名(平均年龄 74.6±8.6 岁)接受胸部 SDCT 检查且有 CIED 植入的患者。重建了 CI、MAR、VMI 和 VMI(10keV 增量,范围:100-200keV)。使用 ROI 确定了 CIED 发生器和导线附近低密度和高密度伪影相邻区域的平均衰减值(HU)和标准差。两名放射科医生对相邻组织的伪影减少和诊断评估进行了定性评估。
与 CI 相比,MAR 和 VMI≥100keV 显著增加了 CIED 发生器和导线周围低密度伪影的衰减,显著降低了高密度伪影的衰减(p<0.05)。仅 VMI≥100keV 可显著降低发生器周围的高密度伪影(p<0.05)。定性分析显示,VMI≥100keV、MAR 和 VMI≥100keV 可显著减少发生器产生的高低密度伪影,并改善周围结构的诊断评估(p<0.05)。MAR 和 VMI 100keV 可改善与导线相邻结构的诊断评估(p<0.05),而 VMI≥140keV 无论是否结合 MAR 均会显著降低诊断评估(p<0.05)。
VMI 和 MAR 相结合以及 MAR 作为独立方法可有效减少 CIED 伪影。但由于沿导线的软组织和血管对比度降低,应谨慎使用更高的 keV 值。
VMI 和 MAR 相结合以及 MAR 作为独立方法可有效减少 CIED 伪影。
由于软组织和血管对比度的损失可能会妨碍诊断评估,因此应谨慎使用 VMI 和 VMI 沿 CIED 导线的较高 keV 值。
CIED 发生器的推荐 keV 值为 140-200keV,导线的推荐 keV 值为 100keV 左右。