Department of Dermatology, Hamamatsu University School of Medicine, Hamamatsu, Japan.
Department of Cellular & Molecular Anatomy, Hamamatsu University School of Medicine, Hamamatsu, Japan.
Front Immunol. 2021 Feb 3;11:618897. doi: 10.3389/fimmu.2020.618897. eCollection 2020.
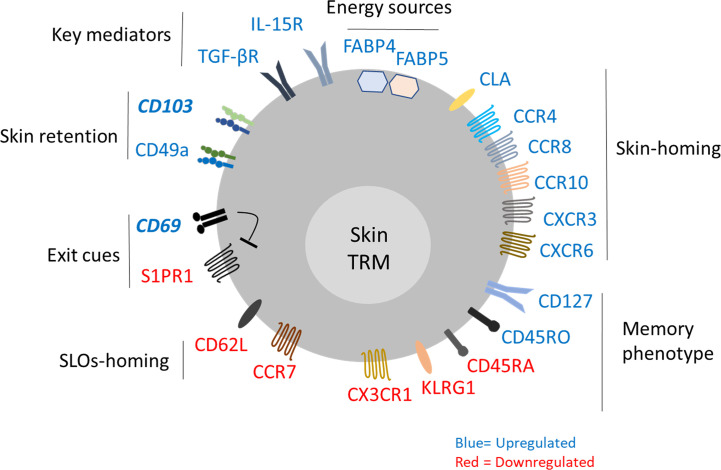
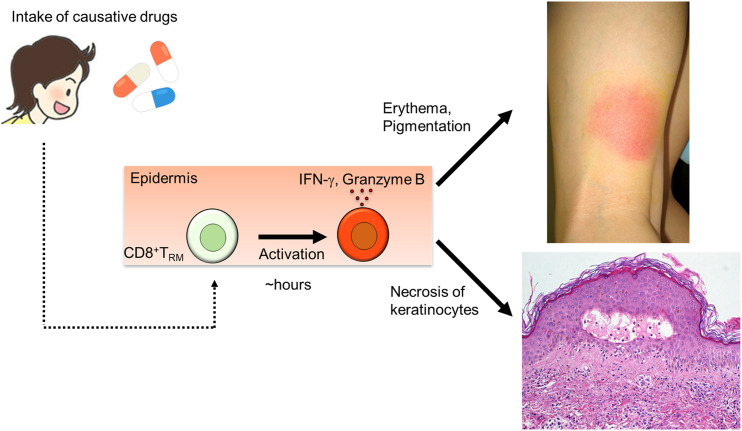
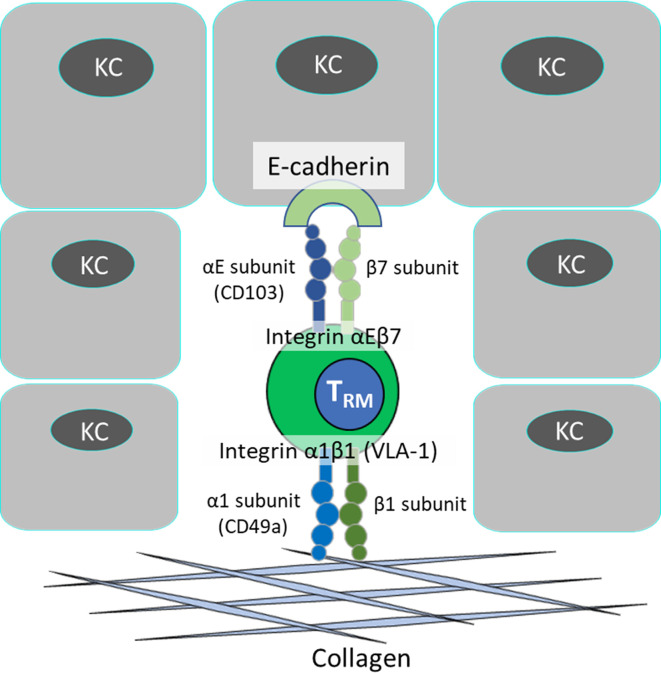
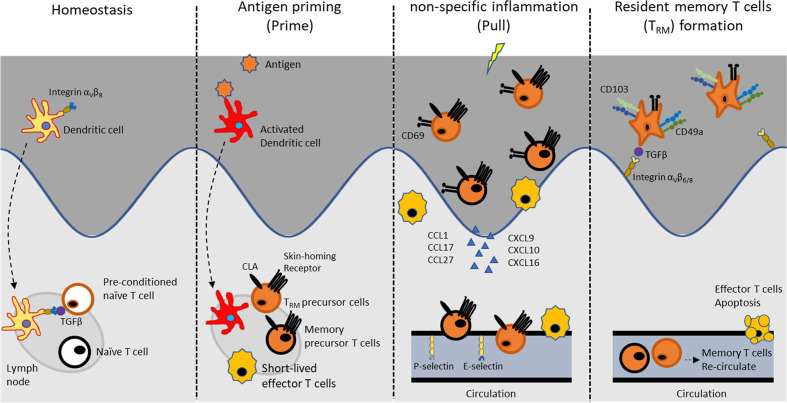
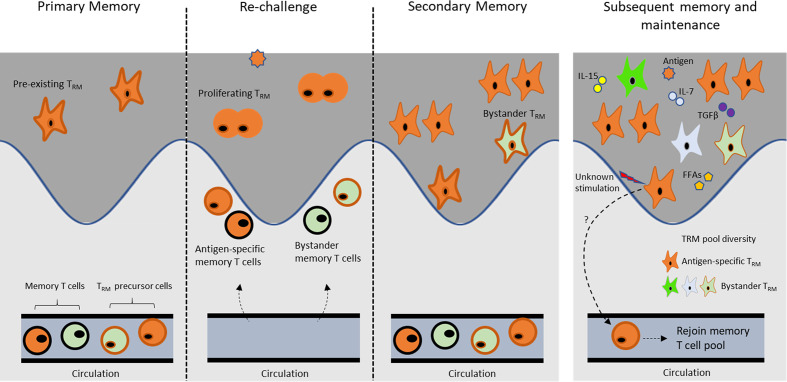
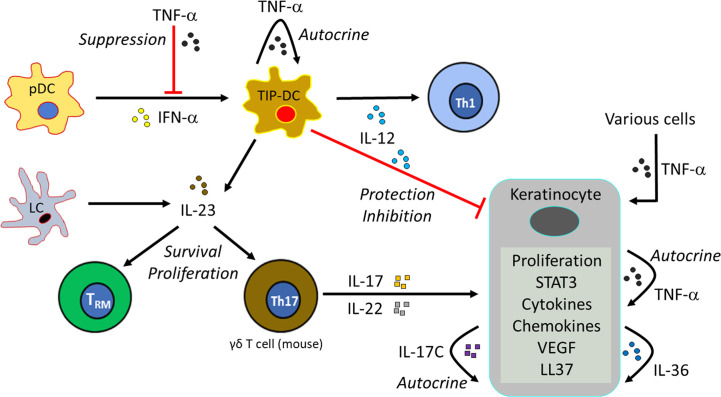
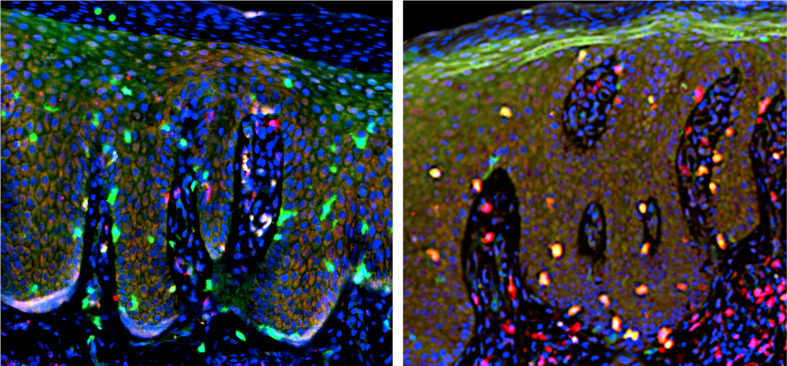
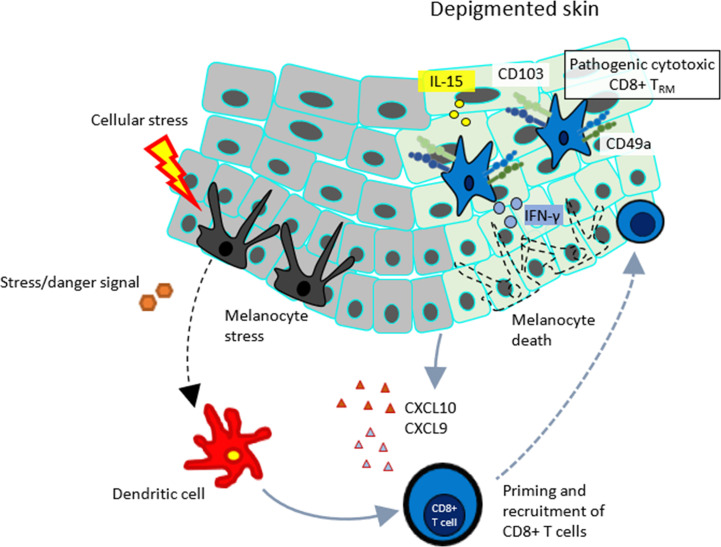
Tissue resident memory T (T) cells reside in peripheral, non-lymphoid tissues such as the skin, where they act as alarm-sensor cells or cytotoxic cells. Physiologically, skin T cells persist for a long term and can be reactivated upon reinfection with the same antigen, thus serving as peripheral sentinels in the immune surveillance network. CD8CD69CD103 T cells are the well-characterized subtype that develops in the epidermis. The local mediators such as interleukin (IL)-15 and transforming growth factor (TGF)-β are required for the formation of long-lived T cell population in skin. Skin T cells engage virus-infected cells, proliferate in response to local antigens and do not migrate out of the epidermis. Secondary T cell populations are derived from pre-existing T cells and newly recruited T precursors from the circulation. In addition to microbial pathogens, topical application of chemical allergen to skin causes delayed-type hypersensitivity and amplifies the number of antigen-specific CD8 T cells at challenged site. Skin T cells are also involved in the pathological conditions, including vitiligo, psoriasis, fixed drug eruption and cutaneous T-cell lymphoma (CTCL). The functions of these T cells seem to be different, depending on each pathology. Psoriasis plaques are seen in a recurrent manner especially at the originally affected sites. Upon stimulation of the skin of psoriasis patients, the CD8CD103CD49a T cells in the epidermis seem to be reactivated and initiate IL-17A production. Meanwhile, autoreactive CD8CD103CD49a T cells secreting interferon-γ are present in lesional vitiligo skin. Fixed drug eruption is another disease where skin T cells evoke its characteristic clinical appearance upon administration of a causative drug. Intraepidermal CD8 T cells with an effector-memory phenotype resident in the skin lesions of fixed drug eruption play a major contributing role in the development of localized tissue damage. CTCL develops primarily in the skin by a clonal expansion of a transformed T cells. CD8 CTCL with the pagetoid epidermotropic histology is considered to originate from epidermal CD8 T cells. This review will discuss the current understanding of skin T biology and their contribution to skin homeostasis and diseases.
组织驻留记忆 T (T) 细胞存在于外周非淋巴组织如皮肤中,作为警报传感器细胞或细胞毒性细胞发挥作用。从生理上讲,皮肤 T 细胞可以长期存在,并在再次感染相同抗原时被重新激活,因此作为免疫监视网络中的外周哨兵。CD8CD69CD103 T 细胞是在表皮中发育的特征明确的亚型。局部介质如白细胞介素 (IL)-15 和转化生长因子 (TGF)-β 是皮肤中形成长寿 T 细胞群体所必需的。皮肤 T 细胞与感染病毒的细胞结合,在局部抗原的刺激下增殖,不会从表皮迁移出去。次级 T 细胞群体来源于预先存在的 T 细胞和从循环中招募的新的 T 前体。除了微生物病原体,化学变应原局部应用于皮肤会引起迟发型超敏反应,并在受挑战部位扩增抗原特异性 CD8 T 细胞的数量。皮肤 T 细胞也参与包括白癜风、银屑病、固定性药物疹和皮肤 T 细胞淋巴瘤 (CTCL) 在内的病理状况。这些 T 细胞的功能似乎因每种病理状况而异。银屑病斑块以反复发作的方式出现,尤其是在最初受影响的部位。在银屑病患者的皮肤受到刺激时,表皮中的 CD8CD103CD49a T 细胞似乎被重新激活并启动 IL-17A 的产生。与此同时,在病变白癜风皮肤中存在分泌干扰素-γ的自身反应性 CD8CD103CD49a T 细胞。固定性药物疹是另一种疾病,皮肤 T 细胞在给予致病药物时会引起其特征性的临床外观。固定性药物疹皮损中的表皮内 CD8 T 细胞具有效应记忆表型,是导致局部组织损伤的主要原因。CTCL 主要通过转化 T 细胞的克隆扩增发生在皮肤中。具有 pagetoid 表皮嗜性组织学特征的 CD8 CTCL 被认为起源于表皮 CD8 T 细胞。本综述将讨论皮肤 T 生物学的最新认识及其对皮肤稳态和疾病的贡献。