Department of Neurology, Seton Dell Medical School Stroke Institute, Austin, Texas, United States.
Department of Health Systems and Population Health Sciences, University of Houston College of Medicine, Houston, Texas, United States.
Thromb Haemost. 2021 Aug;121(8):1097-1106. doi: 10.1055/a-1400-6159. Epub 2021 Apr 14.
Lack of data on balancing bleeding and thrombosis risk causes uncertainty about restarting anticoagulants after major bleeding. Anticoagulant reversal trials offer prospectively gathered data after major bleeding with well-documented safety events and restarting behavior.
To examine the relationship of restarting anticoagulation with thrombosis, rebleeding, and death.
This is a posthoc analysis of a prospective factor Xa inhibitor reversal study at 63 centers in North America and Europe. We compared outcomes of restarted patients with those not restarted using landmark and time-dependent Cox proportional hazards models. Outcomes included thrombotic and bleeding events and death and a composite of all three.
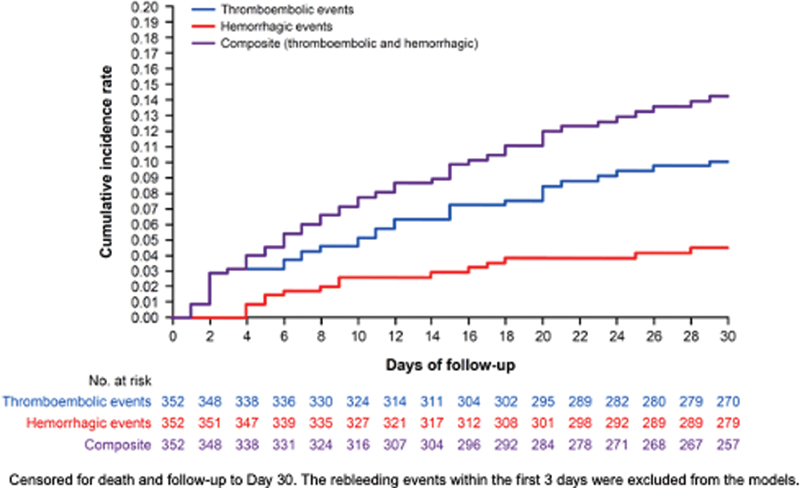
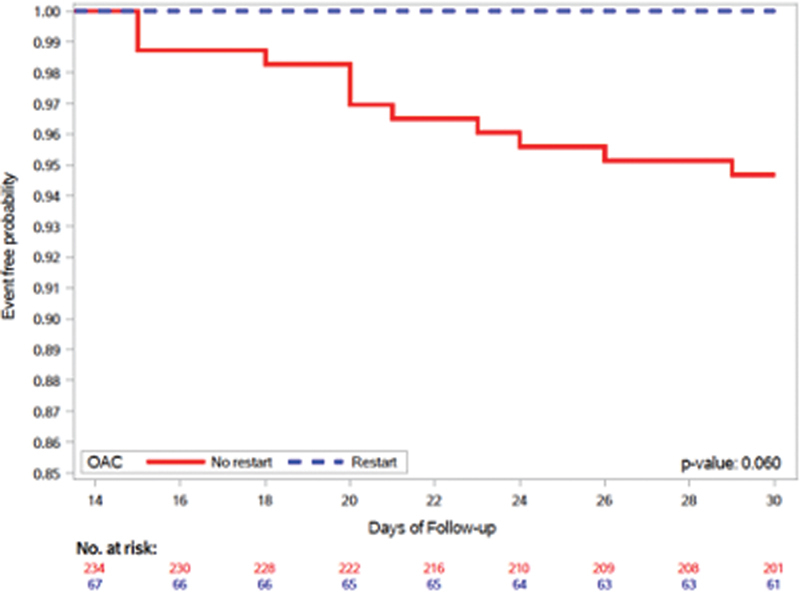
Of 352 patients enrolled, oral anticoagulation was restarted in 100 (28%) during 30-day follow-up. Thirty-four (9.7%) had thrombotic events, 15 (4.3%) had bleeding events (after day 3), and 49 (14%) died. In the landmark analysis comparing patients restarted within 14 days to those not, restarting was associated with decreased thrombotic events (hazard ratio [HR] = 0.112; 95% confidence interval [CI]: 0.001-0.944; = 0.043) and increased rebleeding (HR = 8.39; 95% CI: 1.13-62.29; = 0.037). The time-dependent Cox model showed evidence for a reduction in a composite (thrombotic events, bleeding, and death) attempting to capture net benefit (HR = 0.384; 95% CI: 0.161-0.915; = 0.031).
This analysis provides modest evidence that restarting anticoagulation in factor Xa inhibitor-associated major bleeding patients is correlated with reduced risk of thrombotic events and increased risk of rebleeding. There is low-level evidence of net benefit for restarting. A randomized trial of restarting would be appropriate.
由于缺乏大出血后平衡出血和血栓风险的数据,导致在重新开始抗凝治疗时存在不确定性。抗凝逆转试验提供了在大出血后前瞻性收集的具有良好记录的安全性事件和重新开始治疗行为的数据。
检查重新开始抗凝治疗与血栓形成、再出血和死亡之间的关系。
这是一项在北美和欧洲 63 个中心进行的前瞻性因子 Xa 抑制剂逆转研究的事后分析。我们使用 landmark 和时依 Cox 比例风险模型比较了重新开始治疗的患者与未重新开始治疗的患者的结局。结局包括血栓形成和出血事件以及死亡和三者的复合事件。
在纳入的 352 名患者中,在 30 天随访期间有 100 名(28%)重新开始口服抗凝治疗。34 名(9.7%)发生血栓形成事件,15 名(4.3%)发生出血事件(第 3 天以后),49 名(14%)死亡。在比较 14 天内重新开始治疗的患者和未重新开始治疗的患者的 landmark 分析中,重新开始治疗与血栓形成事件减少相关(风险比 [HR] = 0.112;95%置信区间 [CI]:0.001-0.944; = 0.043),与再出血增加相关(HR = 8.39;95% CI:1.13-62.29; = 0.037)。时依 Cox 模型显示,试图捕捉净获益的复合结局(血栓形成事件、出血和死亡)存在降低的证据(HR = 0.384;95% CI:0.161-0.915; = 0.031)。
这项分析提供了适度的证据表明,在因子 Xa 抑制剂相关的大出血患者中重新开始抗凝治疗与血栓形成事件风险降低和再出血风险增加相关。重新开始治疗有低水平的净获益证据。进行重新开始治疗的随机试验是合适的。