Gianella Fabiola, Hsia Connie Cw, Sakhaee Khashayar
Pulmonary and Critical Care Medicine Division, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Fac Rev. 2020 Nov 18;9:14. doi: 10.12703/b/9-14. eCollection 2020.
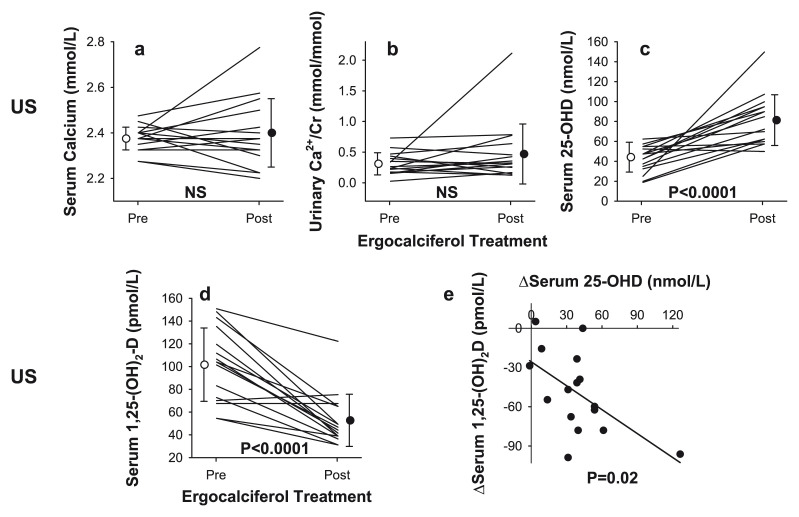
After the initial description of extrarenal synthesis of 1,25-dihydroxyvitamin D (1,25-(OH)D) three decades ago, extensive progress has been made in unraveling the immunomodulatory roles of vitamin D in the pathogenesis of granulomatous disorders, including sarcoidosis. It has been shown that 1,25-(OH)D has dual effects on the immune system, including upregulating innate immunity as well as downregulating the autoimmune response. The latter mechanism plays an important role in the pathogenesis and treatment of sarcoidosis. Vitamin D supplementation in patients with sarcoidosis has been hampered owing to concerns about the development of hypercalcemia and hypercalciuria given that extrarenal 1-α hydroxylase is substrate dependent. Recently, a few studies have cast doubt over the mechanisms underlying the development of hypercalcemia in this population. These studies demonstrated an inverse relationship between the level of vitamin D and severity of sarcoidosis. Consequently, clinical interest has been piqued in the use of vitamin D to attenuate the autoimmune response in this disorder. However, the development of hypercalcemia and the attendant detrimental effects are real possibilities. Although the average serum calcium concentration did not change following vitamin D supplementation, in two recent studies, hypercalciuria occurred in one out of 13 and two out of 16 patients. This review is a concise summary of the literature, outlining past work and newer developments in the use of vitamin D in sarcoidosis. We feel that larger-scale placebo-controlled randomized studies are needed in this population. Since the current first-line treatment of sarcoidosis is glucocorticoids, which confer many systemic adverse effects, and steroid-sparing immunosuppressant treatment options carry additional risks of adverse effects, adjunct management with vitamin D in combination with potent anti-osteoporotic medications could minimize the risk of glucocorticoid-induced osteoporosis and modulate the immune system to attenuate disease activity in sarcoidosis.
三十年前首次描述了1,25 - 二羟基维生素D(1,25-(OH)D)的肾外合成之后,在揭示维生素D在包括结节病在内的肉芽肿性疾病发病机制中的免疫调节作用方面取得了广泛进展。已表明1,25-(OH)D对免疫系统具有双重作用,包括上调固有免疫以及下调自身免疫反应。后一种机制在结节病的发病机制和治疗中起重要作用。鉴于肾外1-α羟化酶是底物依赖性的,结节病患者补充维生素D一直受到高钙血症和高钙尿症发生的担忧的阻碍。最近,一些研究对该人群高钙血症发生的潜在机制提出了质疑。这些研究表明维生素D水平与结节病严重程度之间呈负相关。因此,使用维生素D减轻该疾病自身免疫反应的临床兴趣被激发。然而,高钙血症的发生及随之而来的有害影响是切实可能的。尽管补充维生素D后平均血清钙浓度没有变化,但在最近的两项研究中,13名患者中有1名、16名患者中有2名出现了高钙尿症。这篇综述是对文献的简要总结,概述了过去在结节病中使用维生素D的工作及新进展。我们认为该人群需要开展更大规模的安慰剂对照随机研究。由于目前结节病的一线治疗是糖皮质激素,其会带来许多全身不良反应,且保留类固醇的免疫抑制治疗选择存在额外的不良反应风险,联合使用维生素D与强效抗骨质疏松药物进行辅助治疗可将糖皮质激素诱导的骨质疏松风险降至最低,并调节免疫系统以减轻结节病的疾病活动。