Messas Emmanuel, Goudot Guillaume, Halliday Alison, Sitruk Jonas, Mirault Tristan, Khider Lina, Saldmann Frederic, Mazzolai Lucia, Aboyans Victor
Vascular Medicine Department, Georges Pompidou European Hospital, APHP, Paris, France.
Nuffield Department of Surgical Sciences, University of Oxford, Level 6 John Radcliffe Hospital, Oxford OX3 9DU, UK.
Eur Heart J Suppl. 2020 Dec 6;22(Suppl M):M35-M42. doi: 10.1093/eurheartj/suaa162. eCollection 2020 Nov.
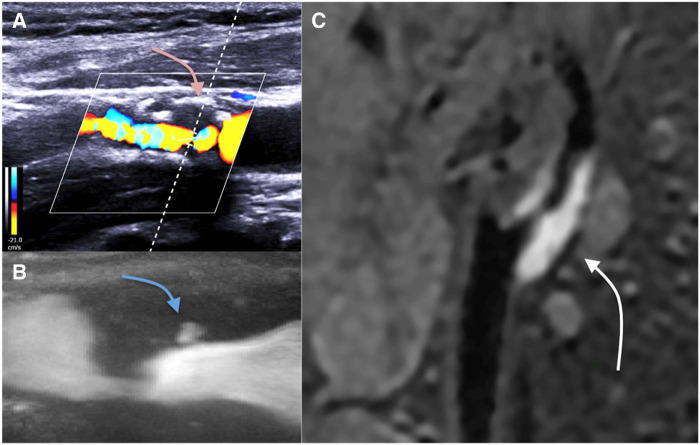
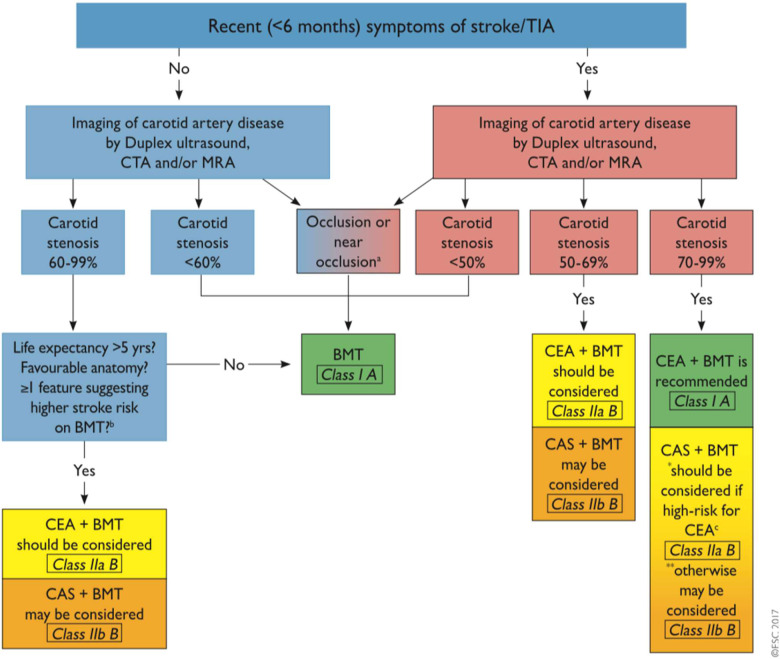
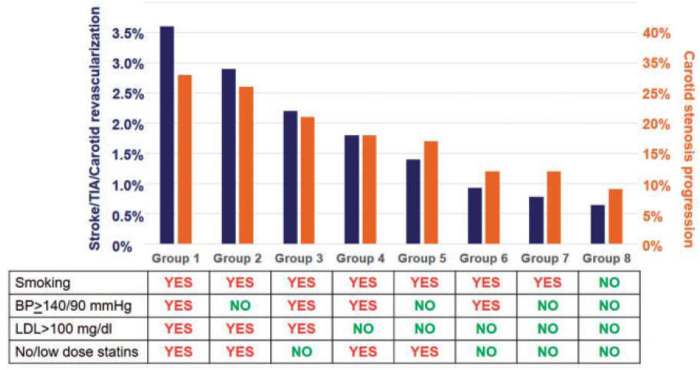
Carotid atherosclerotic plaque is encountered frequently in patients at high cardiovascular risk, especially in the elderly. When plaque reaches 50% of carotid lumen, it induces haemodynamically significant carotid stenosis, for which management is currently at a turning point. Improved control of blood pressure, smoking ban campaigns, and the widespread use of statins have reduced the risk of cerebral infarction to <1% per year. However, about 15% of strokes are still secondary to a carotid stenosis, which can potentially be detected by effective imaging techniques. For symptomatic carotid stenosis, current ESC guidelines put a threshold of 70% for formal indication for revascularization. A revascularization should be discussed for symptomatic stenosis over 50% and for asymptomatic carotid stenosis over 60%. This evaluation should be performed by ultrasound as a first-line examination. As a complement, computed tomography angiography (CTA) and/or magnetic resonance angiography are recommended for evaluating the extent and severity of extracranial carotid stenosis. In perspective, new high-risk markers are currently being developed using markers of plaque neovascularization, plaque inflammation, or plaque tissue stiffness. Medical management of patient with carotid stenosis is always warranted and applied to any patient with atheromatous lesions. Best medical therapy is based on cardiovascular risk factors correction, including lifestyle intervention and a pharmacological treatment. It is based on the tri-therapy strategy with antiplatelet, statins, and ACE inhibitors. The indications for carotid endarterectomy (CEA) and carotid artery stenting (CAS) are similar: for symptomatic patients (recent stroke or transient ischaemic attack ) if stenosis >50%; for asymptomatic patients: tight stenosis (>60%) and a perceived high long-term risk of stroke (determined mainly by imaging criteria). Choice of procedure may be influenced by anatomy (high stenosis, difficult CAS or CEA access, incomplete circle of Willis), prior illness or treatment (radiotherapy, other neck surgery), or patient risk (unable to lie flat, poor AHA assessment). In conclusion, neither systematic nor abandoned, the place of carotid revascularization must necessarily be limited to the plaques at highest risk, leaving a large place for optimized medical treatment as first line management. An evaluation of the value of performing endarterectomy on plaques considered to be at high risk is currently underway in the ACTRIS and CREST 2 studies. These studies, along with the next result of ACST-2 trial, will provide us a more precise strategy in case of carotid stenosis.
颈动脉粥样硬化斑块在心血管高危患者中很常见,尤其是老年人。当斑块占据颈动脉管腔的50%时,就会导致具有血流动力学意义的颈动脉狭窄,目前针对其治疗正处于转折点。血压控制的改善、戒烟运动以及他汀类药物的广泛使用已将脑梗死风险降低至每年<1%。然而,仍有大约15%的中风继发于颈动脉狭窄,而有效的成像技术有可能检测出这种情况。对于有症状的颈动脉狭窄,目前欧洲心脏病学会(ESC)指南将血管重建的正式指征阈值设定为70%。对于症状性狭窄超过50%以及无症状性颈动脉狭窄超过60%的情况,应讨论血管重建问题。这种评估应以超声作为一线检查手段。作为补充,推荐使用计算机断层血管造影(CTA)和/或磁共振血管造影来评估颅外颈动脉狭窄的范围和严重程度。从长远来看,目前正在利用斑块新生血管形成、斑块炎症或斑块组织硬度的标志物开发新的高危标志物。颈动脉狭窄患者的药物治疗始终是必要的,适用于任何患有动脉粥样硬化病变的患者。最佳药物治疗基于对心血管危险因素的纠正,包括生活方式干预和药物治疗。它基于抗血小板、他汀类药物和血管紧张素转换酶(ACE)抑制剂的三联治疗策略。颈动脉内膜切除术(CEA)和颈动脉支架置入术(CAS)的指征相似:对于有症状的患者(近期中风或短暂性脑缺血发作),如果狭窄>50%;对于无症状的患者:严重狭窄(>60%)且存在较高的长期中风风险(主要由影像学标准确定)。手术方式的选择可能会受到解剖结构(高度狭窄、CAS或CEA手术入路困难、Willis环不完整)、既往疾病或治疗(放疗、其他颈部手术)或患者风险(无法平躺、美国心脏协会[ AHA ]评估较差)的影响。总之,颈动脉血管重建既不应一概而论,也不应被摒弃,其应用范围必然要局限于风险最高的斑块,而优化的药物治疗作为一线管理仍有很大的应用空间。目前正在ACTRIS和CREST 2研究中对被认为处于高风险的斑块进行内膜切除术的价值进行评估。这些研究以及ACST - 2试验的下一个结果,将为我们提供在颈动脉狭窄情况下更精确的治疗策略。