Department of Psychiatry, Sinai Health and Lunenfeld Tanenbaum Research Institute, Toronto, Canada.
Department of Psychiatry, Faculty of Medicine, University of Toronto, Toronto, Canada.
Trials. 2021 Mar 5;22(1):186. doi: 10.1186/s13063-021-05075-1.
Depression and anxiety impact up to 1 in 5 pregnant and postpartum women worldwide. Yet, as few as 20% of these women are treated with frontline interventions such as evidence-based psychological treatments. Major barriers to uptake are the limited number of specialized mental health treatment providers in most settings, and problems with accessing in-person care, such as childcare or transportation. Task sharing of treatment to non-specialist providers with delivery on telemedicine platforms could address such barriers. However, the equivalence of these strategies to specialist and in-person models remains unproven.
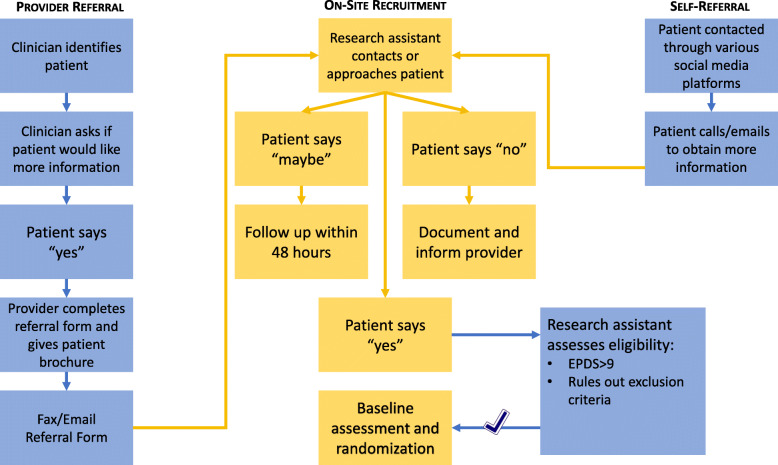
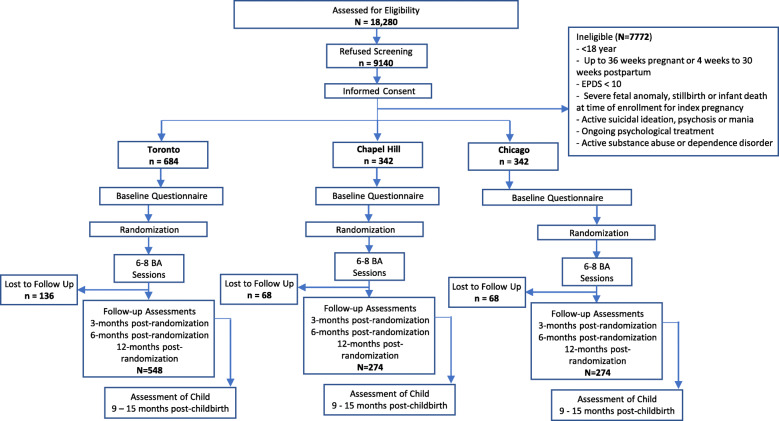
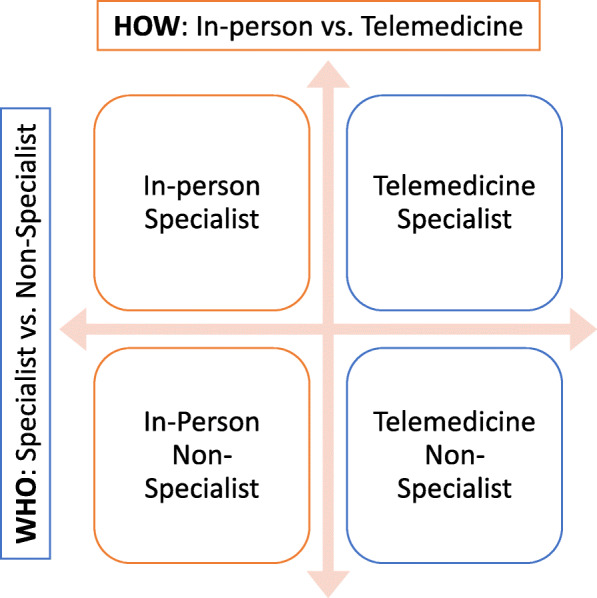
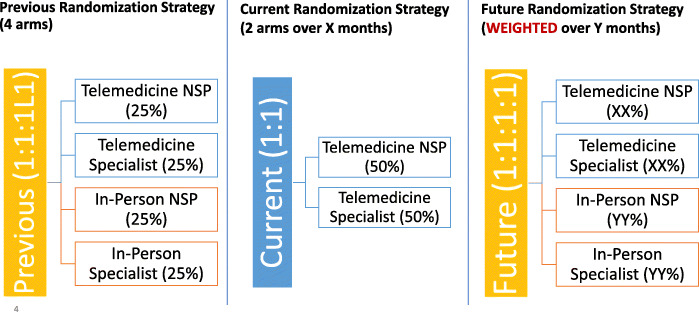
This study protocol outlines the Scaling Up Maternal Mental healthcare by Increasing access to Treatment (SUMMIT) randomized trial. SUMMIT is a pragmatic, non-inferiority test of the comparable effectiveness of two types of providers (specialist vs. non-specialist) and delivery modes (telemedicine vs. in-person) of a brief, behavioral activation (BA) treatment for perinatal depressive and anxiety symptoms. Specialists (psychologists, psychiatrists, and social workers with ≥ 5 years of therapy experience) and non-specialists (nurses and midwives with no formal training in mental health care) were trained in the BA protocol, with the latter supervised by a BA expert during treatment delivery. Consenting pregnant and postpartum women with Edinburgh Postnatal Depression Scale (EPDS) score of ≥ 10 (N = 1368) will be randomized to one of four arms (telemedicine specialist, telemedicine non-specialist, in-person specialist, in-person non-specialist), stratified by pregnancy status (antenatal/postnatal) and study site. The primary outcome is participant-reported depressive symptoms (EPDS) at 3 months post-randomization. Secondary outcomes are maternal symptoms of anxiety and trauma symptoms, perceived social support, activation levels and quality of life at 3-, 6-, and 12-month post-randomization, and depressive symptoms at 6- and 12-month post-randomization. Primary analyses are per-protocol and intent-to-treat. The study has successfully continued despite the COVID-19 pandemic, with needed adaptations, including temporary suspension of the in-person arms and ongoing randomization to telemedicine arms.
The SUMMIT trial is expected to generate evidence on the non-inferiority of BA delivered by a non-specialist provider compared to specialist and telemedicine compared to in-person. If confirmed, results could pave the way to a dramatic increase in access to treatment for perinatal depression and anxiety.
ClinicalTrials.gov NCT04153864 . Registered on November 6, 2019.
全球多达五分之一的孕妇和产后女性受到抑郁和焦虑的影响。然而,这些女性中只有不到 20%接受了循证心理治疗等一线干预措施。接受治疗的主要障碍是大多数环境中专门的心理健康治疗提供者数量有限,以及在获得亲自护理方面存在问题,例如儿童保育或交通。将治疗任务分配给具有远程医疗平台的非专业提供者可能会解决这些障碍。然而,这些策略与专家和亲自治疗模式的等效性仍未得到证实。
本研究方案概述了通过增加治疗机会来扩大孕产妇心理健康服务(SUMMIT)的随机试验。SUMMIT 是一项关于两种提供者(专家与非专家)和两种交付模式(远程医疗与面对面)的简短行为激活(BA)治疗方案对围产期抑郁和焦虑症状的等效性的实用性、非劣效性测试。专家(具有≥ 5 年治疗经验的心理学家、精神科医生和社会工作者)和非专家(具有精神卫生保健正规培训的护士和助产士)接受了 BA 方案的培训,后者在治疗期间由 BA 专家监督。同意参与的孕妇和产后女性(爱丁堡产后抑郁量表(EPDS)评分≥ 10)将被随机分配到四个组之一(远程医疗专家、远程医疗非专家、面对面专家、面对面非专家),按妊娠状态(产前/产后)和研究地点分层。主要结局是参与者在随机分组后 3 个月报告的抑郁症状(EPDS)。次要结局是产妇焦虑和创伤症状、感知社会支持、激活水平以及随机分组后 3、6 和 12 个月的生活质量,以及随机分组后 6 和 12 个月的抑郁症状。主要分析为方案和意向治疗。尽管 COVID-19 大流行,但该研究仍成功继续进行,并进行了必要的调整,包括暂时暂停面对面治疗组和继续随机分配到远程医疗治疗组。
SUMMIT 试验有望生成关于非专家提供者提供的 BA 与专家和远程医疗与面对面相比非劣效性的证据。如果得到证实,结果可能为大幅增加围产期抑郁和焦虑的治疗机会铺平道路。
ClinicalTrials.gov NCT04153864。于 2019 年 11 月 6 日注册。