Université de Paris, PARCC, INSERM U970, 75015, Paris, France.
Laboratoire de Recherches Biochirurgicales (Fondation Carpentier), Assistance Publique-Hôpitaux de Paris (AP-HP), Hôpital Européen Georges Pompidou, Paris, France.
Front Immunol. 2021 Feb 17;11:615240. doi: 10.3389/fimmu.2020.615240. eCollection 2020.
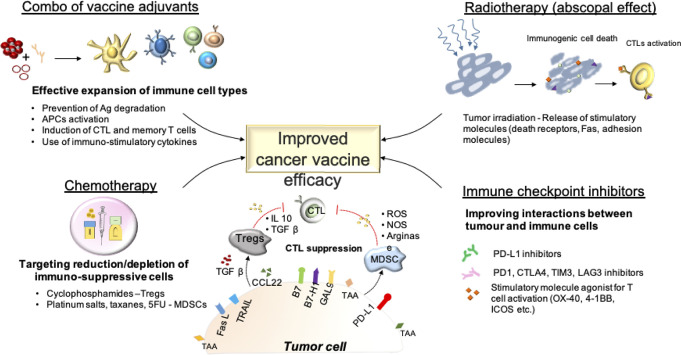
Although the discovery and characterization of multiple tumor antigens have sparked the development of many antigen/derived cancer vaccines, many are poorly immunogenic and thus, lack clinical efficacy. Adjuvants are therefore incorporated into vaccine formulations to trigger strong and long-lasting immune responses. Adjuvants have generally been classified into two categories: those that 'depot' antigens (e.g. mineral salts such as aluminum hydroxide, emulsions, liposomes) and those that act as immunostimulants (Toll Like Receptor agonists, saponins, cytokines). In addition, several novel technologies using vector-based delivery of antigens have been used. Unfortunately, the immune system declines with age, a phenomenon known as immunosenescence, and this is characterized by functional changes in both innate and adaptive cellular immunity systems as well as in lymph node architecture. While many of the immune functions decline over time, others paradoxically increase. Indeed, aging is known to be associated with a low level of chronic inflammation-inflamm-aging. Given that the median age of cancer diagnosis is 66 years and that immunotherapeutic interventions such as cancer vaccines are currently given in combination with or after other forms of treatments which themselves have immune-modulating potential such as surgery, chemotherapy and radiotherapy, the choice of adjuvants requires careful consideration in order to achieve the maximum immune response in a compromised environment. In addition, more clinical trials need to be performed to carefully assess how less conventional form of immune adjuvants, such as exercise, diet and psychological care which have all be shown to influence immune responses can be incorporated to improve the efficacy of cancer vaccines. In this review, adjuvants will be discussed with respect to the above-mentioned important elements.
尽管发现和鉴定了多种肿瘤抗原,激发了许多抗原/衍生的癌症疫苗的开发,但许多抗原的免疫原性较差,因此缺乏临床疗效。因此,佐剂被纳入疫苗制剂中以引发强烈和持久的免疫反应。佐剂通常分为两类:一类是“储存”抗原的佐剂(例如氢氧化铝等矿物盐、乳剂、脂质体),另一类是作为免疫刺激剂的佐剂(Toll 样受体激动剂、皂苷、细胞因子)。此外,还使用了几种基于载体的抗原传递新技术。不幸的是,免疫系统会随着年龄的增长而衰退,这种现象被称为免疫衰老,其特征是先天和适应性细胞免疫系统以及淋巴结结构的功能发生变化。虽然许多免疫功能随着时间的推移而下降,但其他功能却反常地增加。事实上,衰老与慢性低度炎症有关——炎症衰老。鉴于癌症诊断的中位年龄为 66 岁,免疫治疗干预措施(如癌症疫苗)目前与其他具有免疫调节潜力的治疗方法(如手术、化疗和放疗)联合使用或之后使用,因此需要仔细考虑佐剂的选择,以在受损的环境中实现最大的免疫反应。此外,需要进行更多的临床试验来仔细评估不太常规的免疫佐剂形式,如运动、饮食和心理护理,这些都已被证明会影响免疫反应,以提高癌症疫苗的疗效。在这篇综述中,将根据上述重要因素讨论佐剂。