Department of Thoracic Surgery, Peking University People's Hospital, Beijing, 100044, China.
Department of Thoracic Surgery, The Affiliated Cancer Hospital of Zhengzhou University, Henan Cancer Hospital, Zhengzhou, 450008, Henan, China.
J Cancer Res Clin Oncol. 2021 Oct;147(10):3099-3111. doi: 10.1007/s00432-021-03585-8. Epub 2021 Mar 9.
The Prognostic Nutritional Index (PNI), Nutritional Risk Index (NRI), Geriatric Nutritional Risk Index (GNRI), and Controlling Nutritional Status (CONUT) score were devised for quantifying nutritional risk. This study evaluated their properties in detecting compromised nutrition and guiding perioperative management of esophageal cancer patients.
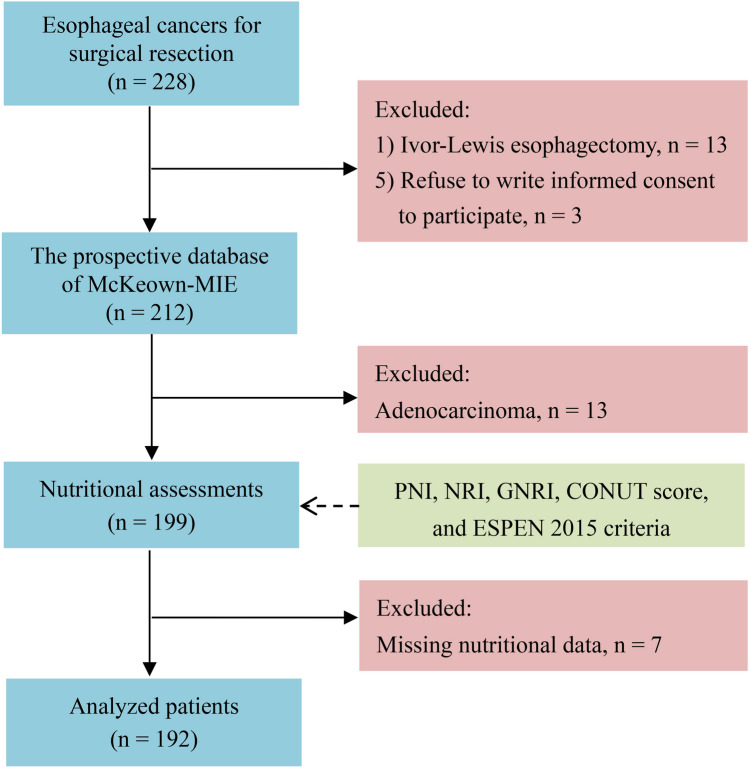
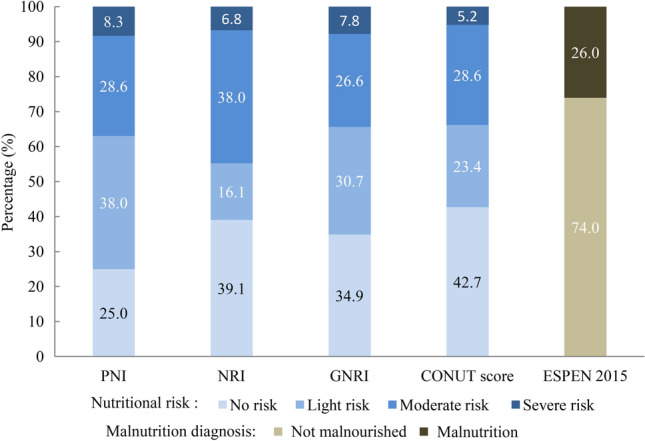
A prospective institutional database of esophageal cancer patients was reviewed and analyzed. Compromised nutritional status was defined as PNI < 50, NRI < 97.5, GNRI < 92, or CONUT score ≥ 4, respectively. The malnutrition diagnosis consensus established by the European Society of Clinical Nutrition and Metabolism (ESPEN 2015) was selected as reference. Multivariable logistic regression and receiver operating characteristic curve analysis were used. External validation was conducted.
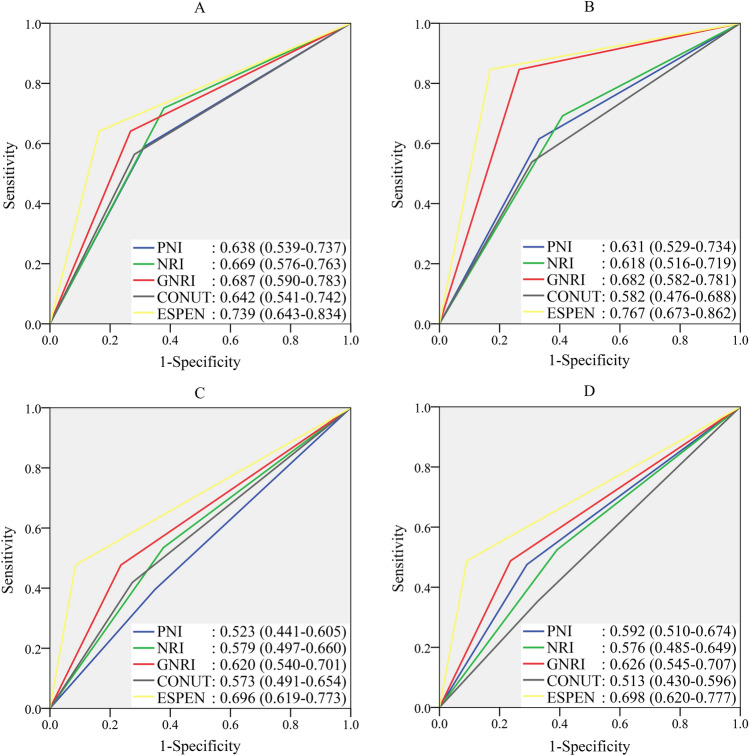
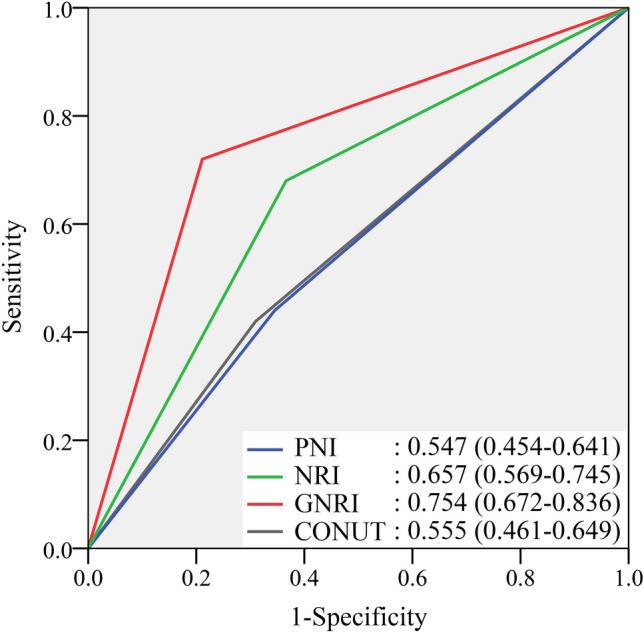
After reviewing the 212-patient database, 192 patients were finally included. Among the four nutritional indexes, the GNRI < 92 showed highest sensitivity (72.0%), specificity (78.9%), and consistency (AUC 0.754, 95% CI 0.672-0.836) with malnutrition diagnosed by ESPEN 2015. The GNRI < 92 showed comparable performance with ESPEN 2015 in recognizing decreased fat mass, fat-free mass, and skeletal muscle mass (all P < 0.01). Both the GNRI < 92 and ESPEN 2015 showed good property in predicting major complications, infectious complications, overall complications and delayed hospital discharge (all P < 0.01), better than PNI < 50, NRI < 97.5, and CONUT score ≥ 4. Regarding the external validation, a retrospective analysis of 155 esophageal cancer patients confirmed the better performance of GNRI < 92 in predicting perioperative morbidities than other 3 nutritional indexes.
The GNRI was optimal in perioperative management of esophageal cancer patients among the four nutritional indexes and was an appropriate alternative to ESPEN 2015 for simplifying nutritional assessment.
预后营养指数(PNI)、营养风险指数(NRI)、老年营养风险指数(GNRI)和控制营养状况(CONUT)评分用于量化营养风险。本研究评估了它们在检测食管癌患者营养受损和指导围手术期管理方面的特性。
回顾性分析了食管癌症患者的前瞻性机构数据库。定义营养状况受损为 PNI<50、NRI<97.5、GNRI<92 或 CONUT 评分≥4。选择欧洲临床营养与代谢学会(ESPEN 2015)制定的营养不良诊断共识作为参考。采用多变量逻辑回归和受试者工作特征曲线分析。进行外部验证。
在审查了 212 例患者的数据库后,最终纳入 192 例患者。在这四个营养指标中,GNRI<92 与 ESPEN 2015 诊断的营养不良具有最高的敏感性(72.0%)、特异性(78.9%)和一致性(AUC 0.754,95%CI 0.672-0.836)。GNRI<92 在识别脂肪量、去脂体重和骨骼肌质量减少方面与 ESPEN 2015 具有相当的性能(均 P<0.01)。GNRI<92 和 ESPEN 2015 均能很好地预测主要并发症、感染性并发症、总并发症和延迟出院(均 P<0.01),优于 PNI<50、NRI<97.5 和 CONUT 评分≥4。关于外部验证,对 155 例食管癌患者的回顾性分析证实,GNRI<92 在预测围手术期并发症方面优于其他 3 种营养指标。
在这四个营养指标中,GNRI 是食管癌患者围手术期管理的最佳指标,是简化营养评估的替代 ESPEN 2015 的合适选择。