Austin Health, 145 Studley Road, Heidelberg, Victoria, 3084, Australia.
Monash Health, Clayton, Australia, Faculty of Medicine, Nursing and Health Science, Monash University, Melbourne, Victoria, Australia.
BMC Anesthesiol. 2021 Mar 10;21(1):74. doi: 10.1186/s12871-021-01281-1.
Enhanced recovery in spinal surgery (ERSS) has shown promising improvements in clinical and economical outcomes. We have proposed an ERSS pathway based on available evidence. We aimed to delineate the clinical efficacy of individual pathway components in ERSS through a systematic narrative review.
We included systematic reviews and meta-analysis, randomized controlled trials, non-randomized controlled studies, and observational studies in adults and pediatric patients evaluating any one of the 22 pre-defined components. Our primary outcomes included all-cause mortality, morbidity outcomes (e.g., pulmonary, cardiac, renal, surgical complications), patient-reported outcomes and experiences (e.g., pain, quality of care experience), and health services outcomes (e.g., length of stay and costs). Following databases (1990 onwards) were searched: MEDLINE, EMBASE, and Cochrane Library (Cochrane Database of Systematic Reviews and CENTRAL). Two authors screened the citations, full-text articles, and extracted data. A narrative synthesis was provided. We constructed Evidence Profile (EP) tables for each component of the pathway, where appropriate information was available. Due to clinical and methodological heterogeneity, we did not conduct a meta-analyses. GRADE system was used to classify confidence in cumulative evidence for each component of the pathway.
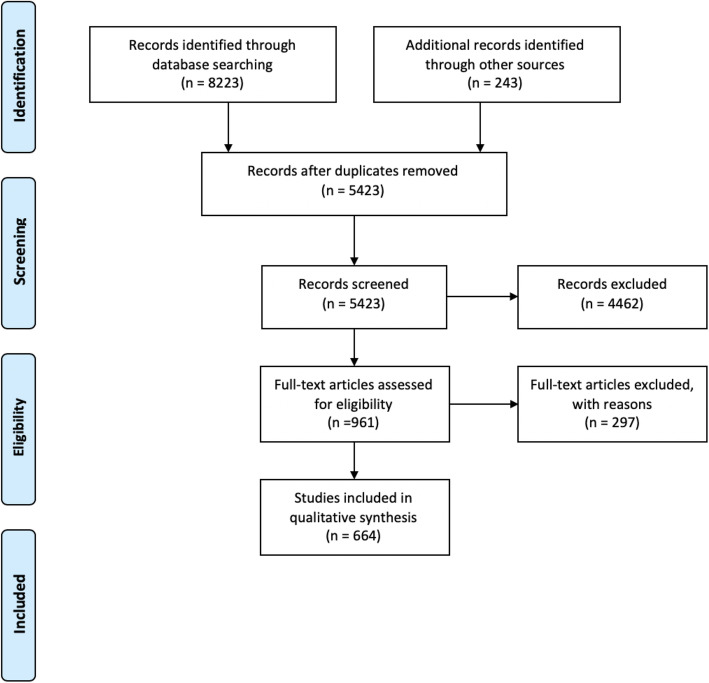
We identified 5423 relevant studies excluding duplicates as relating to the 22 pre-defined components of enhanced recovery in spinal surgery. We included 664 studies in the systematic review. We identified specific evidence within the context of spinal surgery for 14/22 proposed components. Evidence was summarized in EP tables where suitable. We performed thematic synthesis without EP for 6/22 elements. We identified appropriate societal guidelines for the remainder of the components.
We identified the following components with high quality of evidence as per GRADE system: pre-emptive analgesia, peri-operative blood conservation (antifibrinolytic use), surgical site preparation and antibiotic prophylaxis. There was moderate level of evidence for implementation of prehabilitation, minimally invasive surgery, multimodal perioperative analgesia, intravenous lignocaine and ketamine use as well as early mobilization. This review allows for the first formalized evidence-based unified protocol in the field of ERSS. Further studies validating the multimodal ERSS framework are essential to guide the future evolution of care in patients undergoing spinal surgery.
脊柱手术加速康复(ERSS)已显示出在临床和经济结果方面的改善。我们根据现有证据提出了 ERSS 方案。我们旨在通过系统叙述性综述来明确 ERSS 中各个方案组成部分的临床疗效。
我们纳入了评估 22 个预先确定的组成部分之一的成年和儿科患者的系统综述和荟萃分析、随机对照试验、非随机对照研究和观察性研究。我们的主要结局包括全因死亡率、发病率结局(如肺部、心脏、肾脏、手术并发症)、患者报告的结局和体验(如疼痛、护理体验质量)以及卫生服务结局(如住院时间和成本)。检索了以下数据库(1990 年以后):MEDLINE、EMBASE 和 Cochrane 图书馆(Cochrane 系统评价数据库和 CENTRAL)。两名作者筛选了引文、全文文章和提取数据。提供了叙述性综合。我们为该方案的每个组成部分构建了证据概况(EP)表,如果有适当的信息。由于临床和方法学的异质性,我们没有进行荟萃分析。使用 GRADE 系统对该方案每个组成部分的累积证据的置信度进行分类。
我们排除重复项后,共确定了 5423 项与增强型脊柱手术康复的 22 个预先确定组成部分相关的研究。我们在系统综述中纳入了 664 项研究。我们在脊柱手术的背景下确定了 14/22 个提出的组成部分的具体证据。在适当的情况下,我们在 EP 表中总结了证据。我们对 6/22 个要素进行了无 EP 的主题综合。我们为其余组成部分找到了适当的社会指南。
根据 GRADE 系统,我们确定了以下具有高质量证据的组成部分:预防性镇痛、围手术期血液保护(使用抗纤维蛋白溶解剂)、手术部位准备和抗生素预防。实施预康复、微创手术、多模式围手术期镇痛、静脉利多卡因和氯胺酮使用以及早期动员具有中度证据水平。本综述允许在 ERSS 领域首次进行正式的循证统一方案。进一步验证多模式 ERSS 框架的研究对于指导脊柱手术患者未来护理的发展至关重要。