Ji Limei, Jin Lanying, Zheng Shunjie, Shao Mingjun, Cui Dawei, Hu Min
Department of Obstetrics and Gynecology, Jinhua Municipal Central Hospital, Jinhua, China.
Geburtshilfe Frauenheilkd. 2021 Mar;81(3):321-330. doi: 10.1055/a-1337-2690. Epub 2021 Mar 5.
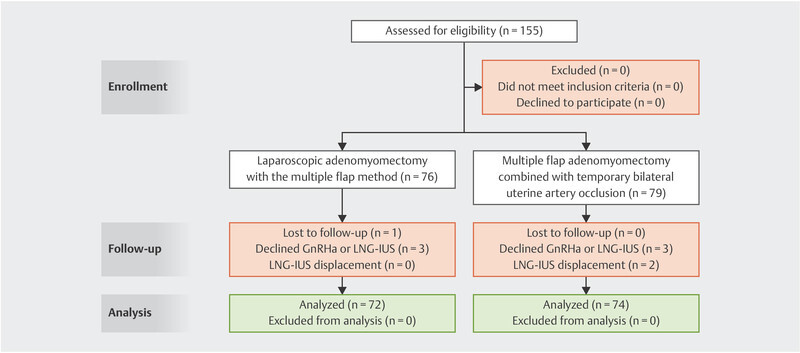
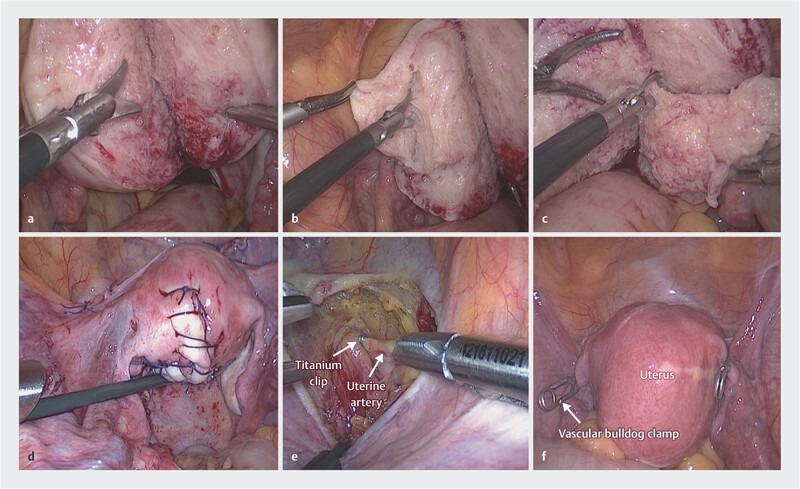
Adenomyomectomy is the most conservative surgical treatment for adenomyosis. However, the surgical efficacy of this treatment and the best approach to use are still debated. We aimed to evaluate the efficacy of laparoscopic adenomyomectomy using the double/multiple-flap method combined with temporary occlusion of the bilateral uterine artery and the utero-ovarian vessels to treat symptomatic adenomyosis. We recruited 155 patients with symptomatic adenomyosis and divided them into group A (n = 76) and group B (n = 79), with each group treated using a different surgical approach. All eligible women were informed of the potential complications, benefits, and alternatives of each approach before they were assigned into one of the two groups. In group A, we performed laparoscopic adenomyomectomy with the double/multiple-flap method while in group B, we performed a double/multiple-flap adenomyomectomy combined with temporary occlusion of the bilateral uterine artery and utero-ovarian vessels. Over a 24-month follow-up period, we evaluated operating time, intraoperative blood loss, visual analog scale (VAS) scores, anti-Mullerian hormone levels, uterine volume, and relief of menorrhagia. There were no significant differences between groups A and B with respect to VAS scores, relief of menorrhagia and uterine volume at 3 months, 6 months, 12 months and 24 months after surgery (p > 0.05). Both groups showed significant improvement of these parameters after surgery compared with preoperative values (p < 0.05). Blood loss in group B was significantly lower than in group A (p < 0.001) while there was no significant difference in operating times (p > 0.05). Levels of AMH did not differ significantly between the groups throughout the follow-up period (p > 0.05). Laparoscopic adenomyomectomy with temporary occlusion of the bilateral uterine artery and the utero-ovarian vessels offers a feasible surgical option to treat symptomatic adenomyoma.
子宫腺肌病病灶切除术是治疗子宫腺肌病最保守的手术方法。然而,这种治疗方法的手术疗效以及最佳手术方式仍存在争议。我们旨在评估采用双瓣/多瓣法联合双侧子宫动脉及子宫卵巢血管临时阻断术的腹腔镜子宫腺肌病病灶切除术治疗有症状子宫腺肌病的疗效。我们招募了155例有症状的子宫腺肌病患者,将其分为A组(n = 76)和B组(n = 79),每组采用不同的手术方法进行治疗。所有符合条件的女性在被分配到两组之一之前,均被告知每种方法的潜在并发症、益处及替代方案。A组采用双瓣/多瓣法进行腹腔镜子宫腺肌病病灶切除术,而B组则采用双瓣/多瓣子宫腺肌病病灶切除术联合双侧子宫动脉及子宫卵巢血管临时阻断术。在24个月的随访期内,我们评估了手术时间、术中出血量、视觉模拟评分(VAS)、抗苗勒管激素水平、子宫体积以及月经过多的缓解情况。术后3个月、6个月、12个月和24个月时,A组和B组在VAS评分、月经过多缓解情况及子宫体积方面无显著差异(p>0.05)。与术前值相比,两组术后这些参数均有显著改善(p<0.05)。B组的出血量显著低于A组(p<0.001),而手术时间无显著差异(p>0.05)。在整个随访期内,两组的抗苗勒管激素水平无显著差异(p>0.05)。腹腔镜子宫腺肌病病灶切除术联合双侧子宫动脉及子宫卵巢血管临时阻断术为治疗有症状的子宫腺肌瘤提供了一种可行的手术选择。