Mesregah Mohamed Kamal, Formanek Blake, Liu John C, Buser Zorica, Wang Jeffrey C
Department of Orthopaedic Surgery, 12223Keck School of Medicine, University of Southern California, Los Angeles, CA, USA.
Department of Orthopaedic Surgery, Menoufia University Faculty of Medicine, Shebin El-Kom, Menoufia, Egypt.
Global Spine J. 2023 Mar;13(2):432-442. doi: 10.1177/2192568221998306. Epub 2021 Mar 12.
Retrospective comparative study.
To compare the perioperative complications of propensity score-matched cohorts of patients with degenerative cervical myelopathy (DCM), who were treated with anterior cervical discectomy and fusion (ACDF), posterior laminectomy with fusion, or laminoplasty.
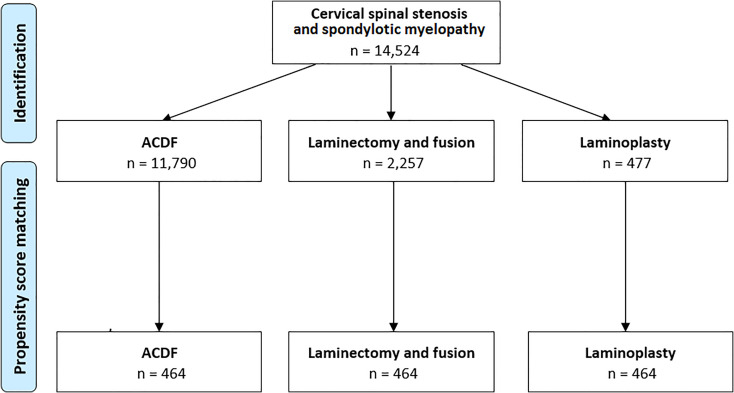
The Humana PearlDiver Patient Record Database was queried using the International Classification of Diseases (ICD-9 and ICD-10) and the Current Procedural Terminology (CPT) codes. Propensity score-matched analysis was done using multiple Chi-squared tests with Bonferroni correction of the significance level.
Cohorts of 11,790 patients who had ACDF, 2,257 patients who had posterior laminectomy with fusion, and 477 patients who had laminoplasty, were identified. After propensity score matching, all the 3 groups included 464 patients. The incidence of dysphagia increased significantly following ACDF compared to laminoplasty, < 0.001, and in laminectomy with fusion compared to laminoplasty, < 0.001. The incidence of new-onset cervicalgia was higher in ACDF compared to laminoplasty, = 0.005, and in laminectomy with fusion compared to laminoplasty, = 0.004. The incidence of limb paralysis increased significantly in laminectomy with fusion compared to ACDF, = 0.002. The revision rate at 1 year increased significantly in laminectomy with fusion compared to laminoplasty, < 0.001, and in ACDF compared to laminoplasty, < 0.001.
The incidence of dysphagia following laminectomy with fusion was not different compared to ACDF. Postoperative new-onset cervicalgia and revisions were least common in laminoplasty. The highest rate of postoperative limb paralysis was noticed in laminectomy with fusion.
回顾性比较研究。
比较经倾向性评分匹配的退变性颈椎病(DCM)患者队列的围手术期并发症,这些患者接受了颈椎前路椎间盘切除融合术(ACDF)、后路椎板切除融合术或椎板成形术。
使用国际疾病分类(ICD - 9和ICD - 10)及现行手术操作术语(CPT)编码查询Humana PearlDiver患者记录数据库。采用多次卡方检验并进行Bonferroni显著性水平校正进行倾向性评分匹配分析。
确定了11790例行ACDF的患者队列、2257例行后路椎板切除融合术的患者队列和477例行椎板成形术的患者队列。经倾向性评分匹配后,三组各纳入464例患者。与椎板成形术相比,ACDF后吞咽困难发生率显著增加,<0.001;与椎板成形术相比,后路椎板切除融合术后吞咽困难发生率也显著增加,<0.001。与椎板成形术相比,ACDF后新发颈痛发生率更高,=0.005;与椎板成形术相比,后路椎板切除融合术后新发颈痛发生率也更高,=0.004。与ACDF相比,后路椎板切除融合术后肢体麻痹发生率显著增加,=0.002。与椎板成形术相比,后路椎板切除融合术1年翻修率显著增加,<0.001;与椎板成形术相比,ACDF的1年翻修率也显著增加,<0.001。
后路椎板切除融合术后吞咽困难发生率与ACDF相比无差异。椎板成形术术后新发颈痛和翻修最少见。后路椎板切除融合术术后肢体麻痹发生率最高。