Malik Astha, Thanekar Unmesha, Amarachintha Surya, Mourya Reena, Nalluri Shreya, Bondoc Alexander, Shivakumar Pranavkumar
Division of Gastroenterology, Hepatology and Nutrition, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States.
Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH, United States.
Front Oncol. 2021 Feb 24;10:627701. doi: 10.3389/fonc.2020.627701. eCollection 2020.
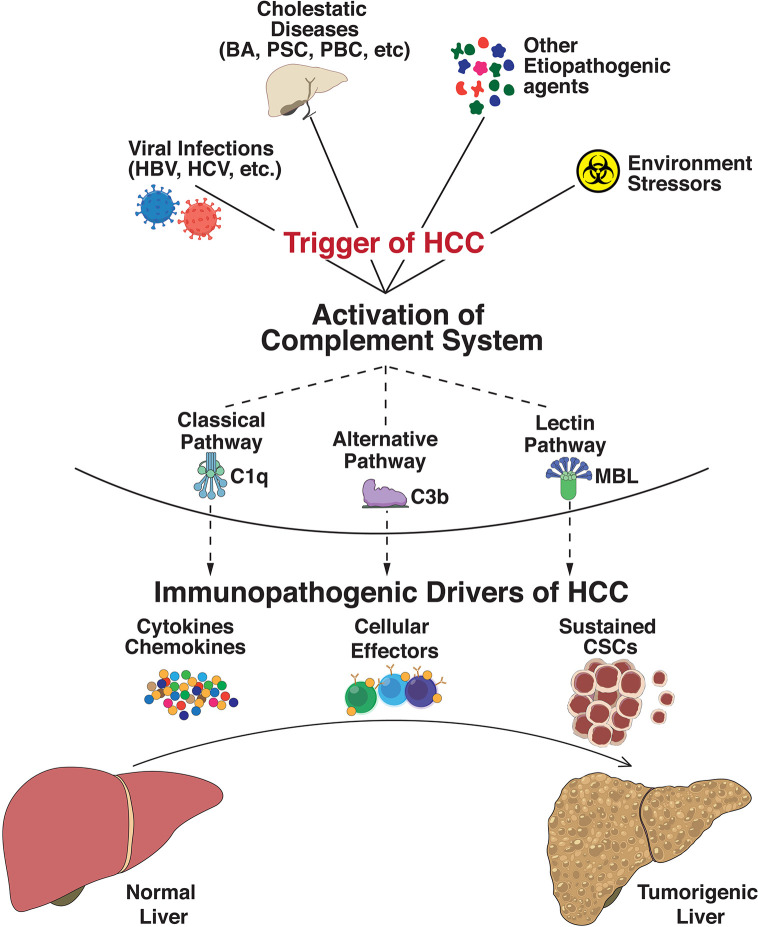
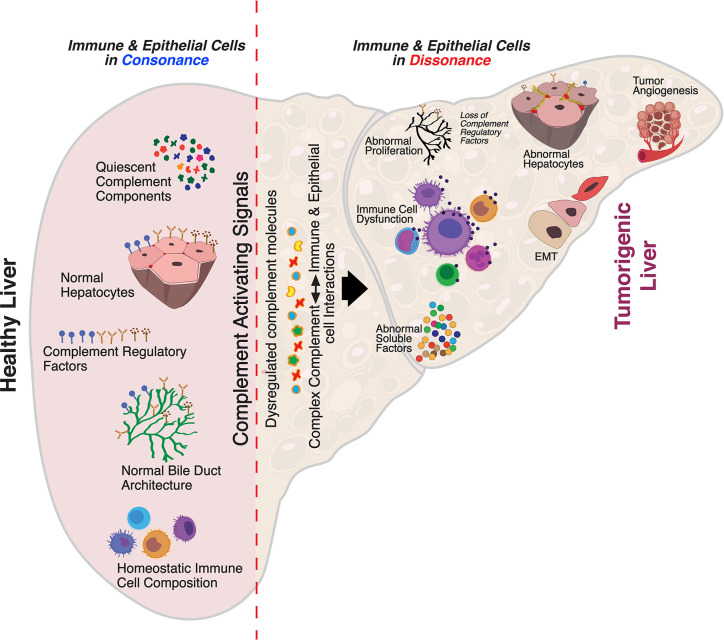
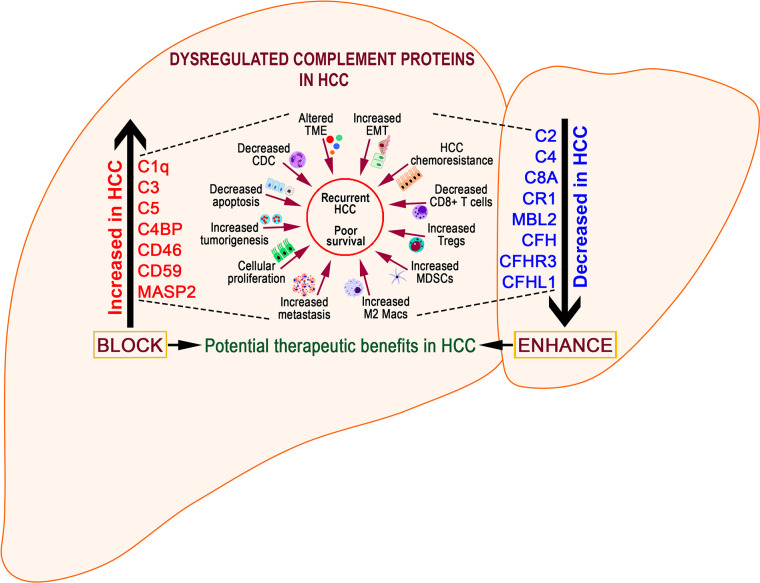
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver and a leading cause of death in the US and worldwide. HCC remains a global health problem and is highly aggressive with unfavorable prognosis. Even with surgical interventions and newer medical treatment regimens, patients with HCC have poor survival rates. These limited therapeutic strategies and mechanistic understandings of HCC immunopathogenesis urgently warrant non-palliative treatment measures. Irrespective of the multitude etiologies, the liver microenvironment in HCC is intricately associated with chronic necroinflammation, progressive fibrosis, and cirrhosis as precedent events along with dysregulated innate and adaptive immune responses. Central to these immunological networks is the complement cascade (CC), a fundamental defense system inherent to the liver which tightly regulates humoral and cellular responses to noxious stimuli. Importantly, the liver is the primary source for biosynthesis of >80% of complement components and expresses a variety of complement receptors. Recent studies implicate the complement system in liver inflammation, abnormal regenerative responses, fibrosis, carcinogenesis, and development of HCC. Although complement activation differentially promotes immunosuppressive, stimulant, and angiogenic microenvironments conducive to HCC development, it remains under-investigated. Here, we review derangement of specific complement proteins in HCC in the context of altered complement regulatory factors, immune-activating components, and their implications in disease pathogenesis. We also summarize how complement molecules regulate cancer stem cells (CSCs), interact with complement-coagulation cascades, and provide therapeutic opportunities for targeted intervention in HCC.
肝细胞癌(HCC)是肝脏最常见的原发性恶性肿瘤,也是美国及全球主要的死亡原因。HCC仍然是一个全球性的健康问题,具有高度侵袭性且预后不良。即使采用手术干预和更新的药物治疗方案,HCC患者的生存率仍很低。这些有限的治疗策略以及对HCC免疫发病机制的认识,迫切需要非姑息性治疗措施。无论病因众多,HCC中的肝脏微环境都与慢性坏死性炎症、进行性纤维化和肝硬化密切相关,这些是先前的事件,同时伴有先天和适应性免疫反应失调。这些免疫网络的核心是补体级联反应(CC),这是肝脏固有的一种基本防御系统,可严格调节对有害刺激的体液和细胞反应。重要的是,肝脏是超过80%补体成分生物合成的主要来源,并表达多种补体受体。最近的研究表明补体系统与肝脏炎症、异常再生反应、纤维化、致癌作用以及HCC的发展有关。虽然补体激活以不同方式促进有利于HCC发展的免疫抑制、刺激和血管生成微环境,但这方面仍研究不足。在这里,我们在补体调节因子、免疫激活成分改变的背景下,综述HCC中特定补体蛋白的紊乱情况及其在疾病发病机制中的意义。我们还总结了补体分子如何调节癌症干细胞(CSC),与补体 - 凝血级联反应相互作用,以及为HCC的靶向干预提供治疗机会。