Marino Achille, Cimaz Rolando, Pelagatti Maria Antonietta, Tattesi Giulia, Biondi Andrea, Menni Laura, Sala Marco, Calzi Patrizia, Morandi Francesco, Cortinovis Francesca, Cogliardi Anna, Addis Claudia, Bellù Roberto, Andreotti Massimo, Varisco Tiziana
Department of Pediatrics, Desio Hospital, Azienda Socio Sanitaria Territoriale Monza, Monza, Italy.
Azienda Socio Sanitaria Territoriale G.Pini-Centro Traumatologico Ortopedico, Milan, Italy.
Front Med (Lausanne). 2021 Feb 24;8:621668. doi: 10.3389/fmed.2021.621668. eCollection 2021.
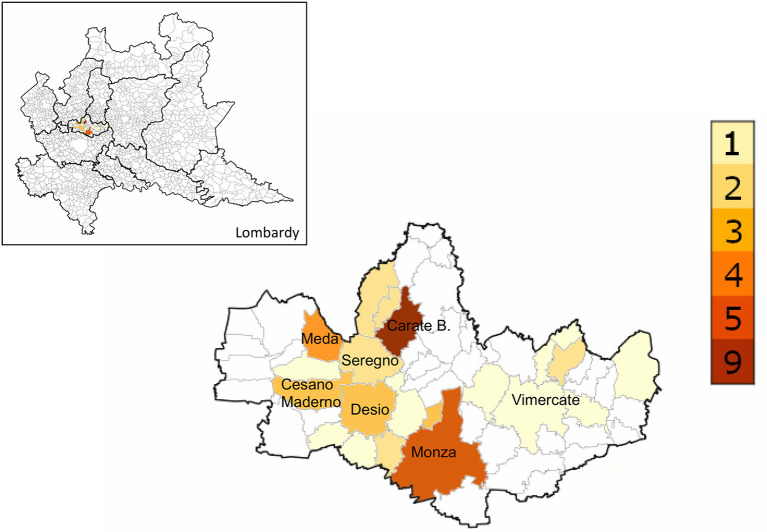
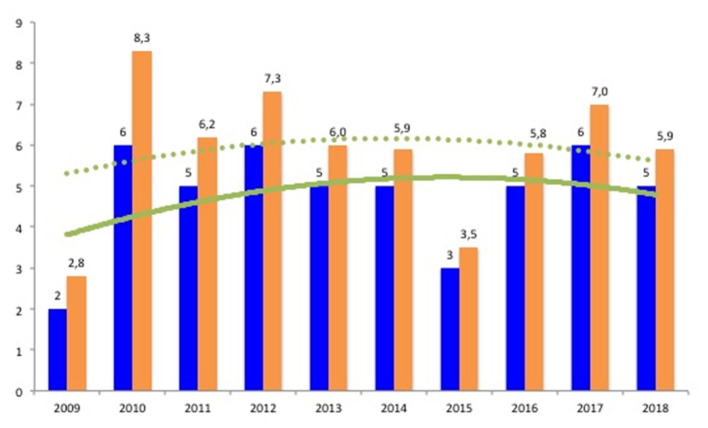
Acute rheumatic fever (ARF) is a non-septic complication of group A β-hemolytic streptococcal (GAS) throat infection. Since 1944, ARF diagnosis relies on the Jones criteria, which were periodically revised. The 2015 revision of Jones criteria underlines the importance of knowing the epidemiological status of its own region with updated data. This study aims to describe ARF features in a retrospective cohort retrieved over a 10-year timespan (2009-2018) and to report the annual incidence of ARF among children in the Province of Monza-Brianza, Lombardy, Italy during the same period. This is a multicentric cross-sectional/retrospective study; 70 patients (39 boys) were diagnosed with ARF. The median age at diagnosis was 8.5 years (range, 4-14.2 years). Overall, carditis represented the most reported major Jones criteria followed by arthritis and chorea (40, 27, and 20 cases, respectively). In order to calculate the annual incidence of ARF, only children resident in the Province of Monza-Brianza were included in this part of the analysis. Therefore, 47 patients aged between 5 and 14 years were identified. The median incidence during the study time was 5.7/100,000 (range, 2.8-8.3/100,000). In the Province of Monza-Brianza, we found an incidence rate of ARF among children aged 5-14 years constantly above the threshold of low-risk area as defined in the 2015 revision of Jones criteria. Therefore, the diagnosis of ARF should be based on the moderate-high-risk set of Jones criteria. However, given the burden of secondary prophylaxis, expert opinion is advisable when the diagnosis of ARF is uncertain.
急性风湿热(ARF)是A组β溶血性链球菌(GAS)咽喉感染的非化脓性并发症。自1944年以来,ARF的诊断依赖于琼斯标准,该标准定期进行修订。2015年琼斯标准的修订强调了根据最新数据了解本地区流行病学状况的重要性。本研究旨在描述在10年时间跨度(2009 - 2018年)内回顾性队列中ARF的特征,并报告同期意大利伦巴第大区蒙扎 - 布里安扎省儿童ARF的年发病率。这是一项多中心横断面/回顾性研究;70例患者(39名男孩)被诊断为ARF。诊断时的中位年龄为8.5岁(范围4 - 14.2岁)。总体而言,心脏炎是报告最多的主要琼斯标准,其次是关节炎和舞蹈病(分别为40例、27例和20例)。为了计算ARF的年发病率,本分析仅纳入居住在蒙扎 - 布里安扎省的儿童。因此,确定了47例年龄在5至14岁之间的患者。研究期间的中位发病率为5.7/100,000(范围2.8 - 8.3/100,000)。在蒙扎 - 布里安扎省,我们发现5至14岁儿童的ARF发病率持续高于2015年琼斯标准修订版中定义的低风险地区阈值。因此,ARF的诊断应基于中度 - 高风险的琼斯标准集。然而,考虑到二级预防的负担,当ARF诊断不确定时,建议咨询专家意见。