Marcus Stroke & Neuroscience Center, Grady Memorial Hospital, Emory University, Atlanta, Georgia, USA.
Department of Mechanical Engineering, National University of Ireland Galway, Galway, Ireland.
J Neurointerv Surg. 2022 Feb;14(2):184-188. doi: 10.1136/neurintsurg-2021-017316. Epub 2021 Mar 15.
Balloon guide catheters (BGCs) achieve proximal flow control during thrombectomy but antegrade intracranial flow often persists via the Circle of Willis. Closely sizing an aspiration catheter to the target vessel might achieve greater flow control and improve technical performance. Our objective was to measure the impact of aspiration catheter size on distal flow control and flow reversal with and without the use of BGCs. Clot retrieval testing was performed to establish the impact of these parameters on revascularization.
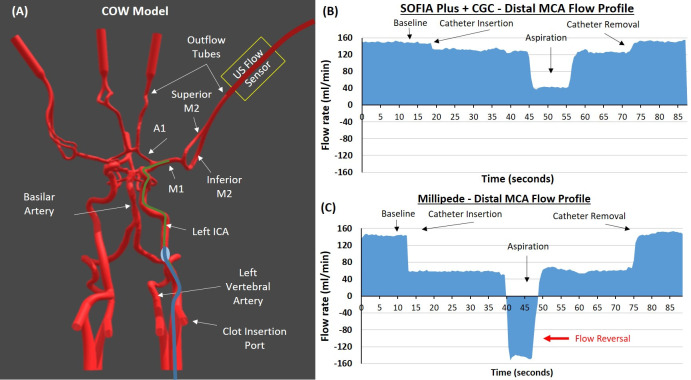
An in vitro thrombectomy model replicated in vivo conditions. Flow was measured continuously using ultrasonic flow sensors placed 20 cm distal to the catheter tip in the middlel cerebral artery (MCA). Four aspiration catheters of increasing size were evaluated: ACE 60 and 64 (Penumbra), SOFIA Plus (MicroVention), and Millipede 088 (Perfuze). Two clot analog types (red blood cell-rich and fibrin/platelet-rich) were used for clot retrieval testing.
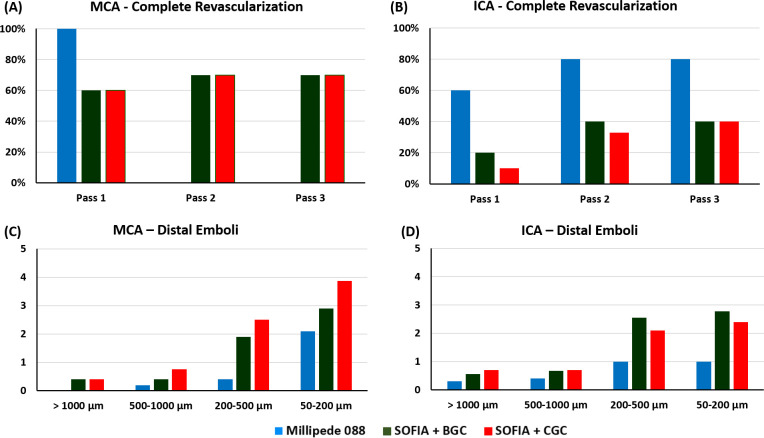
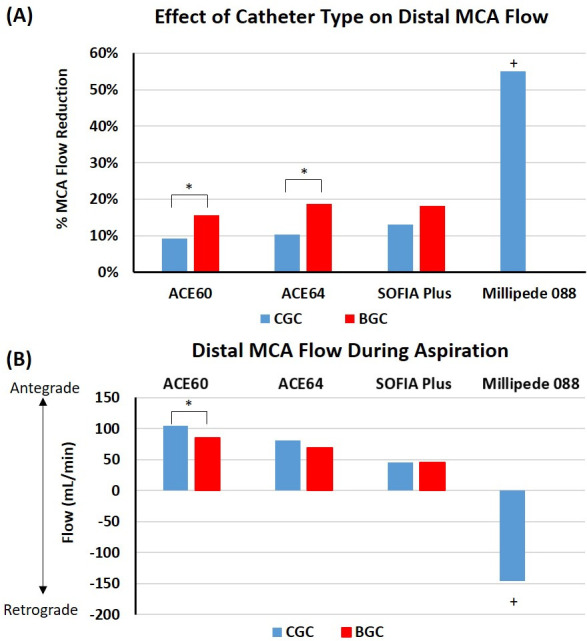
The larger area of the 'superbore' Millipede 088 catheter resulted in a larger reduction in antegrade flow than standard aspiration catheters, even when the latter were combined with a BGC. During aspiration, 6Fr catheters were unable to cause flow reversal in the distal MCA while the Millipede 088 achieved significant distal flow reversal (-146 mL/min) (P<0.0001*) (denotes significance). The solo use of Millipede 088 resulted in better recanalization outcomes and significantly reduced distal emboli for internal carotid artery (P=0.015) and MCA (P=0.014*) occlusions compared with all other devices and combinations.
Maximizing the catheter-to-vessel size facilitates near flow-arrest on catheter insertion, potentially negating the need for a BGC. A 0.088 inch aspiration catheter enables significant flow reversal in the distal MCA during aspiration.
球囊引导导管(BGC)在取栓过程中可实现近端血流控制,但通过 Willis 环,颅内前向血流通常仍持续存在。将抽吸导管与靶血管紧密匹配可能会实现更好的血流控制,提高技术性能。我们的目标是测量抽吸导管大小对远端血流控制和有无 BGC 时血流逆转的影响。通过血栓切除术测试来确定这些参数对再通的影响。
在体外复制了一种与体内条件相似的血栓切除术模型。通过放置在距导管尖端 20cm 的大脑中动脉(MCA)中部的超声流量传感器连续测量流量。评估了 4 种不同尺寸的抽吸导管:ACE 60 和 64(Penumbra)、SOFIA Plus(MicroVention)和 Millipede 088(Perfuze)。两种不同的血栓模拟类型(富含红细胞和富含纤维蛋白/血小板)用于血栓切除术测试。
较大的“超级孔”Millipede 088 导管的面积导致前向血流的减少大于标准抽吸导管,即使后者与 BGC 结合使用也是如此。在抽吸过程中,6Fr 导管无法在远端 MCA 中引起血流逆转,而 Millipede 088 导管则实现了显著的远端血流逆转(-146mL/min)(P<0.0001*)(表示具有统计学意义)。与所有其他装置和组合相比,单独使用 Millipede 088 可实现更好的再通效果,并显著减少颈内动脉(P=0.015)和 MCA(P=0.014*)闭塞的远端栓塞。
导管与血管尺寸的最大化有助于导管插入时的近流阻断,可能无需 BGC。0.088 英寸的抽吸导管可在抽吸过程中使远端 MCA 内产生显著的血流逆转。