Surie Diya, Huang Jennifer Y, Brown Allison C, Gable Paige, Biedron Caitlin, Gilbert Sarah E, Garner Kelley, Bollinger Susan, Gulley Trent, Haney Tafarra, Lyons Amanda K, Beshearse Elizabeth, Gregory Christopher J, Sabour Sarah, Clemmons Nakia S, James Allison E, Tamin Azaibi, Reese Natashia, Perry-Dow K Allison, Brown Robin, Harcourt Jennifer L, Campbell Davina, Houston Hollis, Chakravorty Rohan, Paulick Ashley, Whitaker Brett, Murdoch Jordan, Spicer Lori, Stumpf Megan M, Mills Lisa, Coughlin Melissa M, Higdem Pamela, Rasheed Mohammad Ata Ur, Lonsway David, Bhatnagar Amelia, Kothari Atul, Anderson Karen, Thornburg Natalie J, Breaker Erin, Adamczyk Michelle, McAllister Gillian A, Halpin Alison L, Seely Kathryn A, Patil Naveen, McDonald L Clifford, Kutty Preeta K
COVID-19 Response Team, Centers for Disease Control and Prevention, Atlanta, Georgia, USA.
Arkansas Department of Health, Little Rock, Arkansas, USA.
Open Forum Infect Dis. 2021 Jan 30;8(3):ofab048. doi: 10.1093/ofid/ofab048. eCollection 2021 Mar.
To estimate the infectious period of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in older adults with underlying conditions, we assessed duration of coronavirus disease 2019 (COVID-19) symptoms, reverse-transcription polymerase chain reaction (RT-PCR) positivity, and culture positivity among nursing home residents.
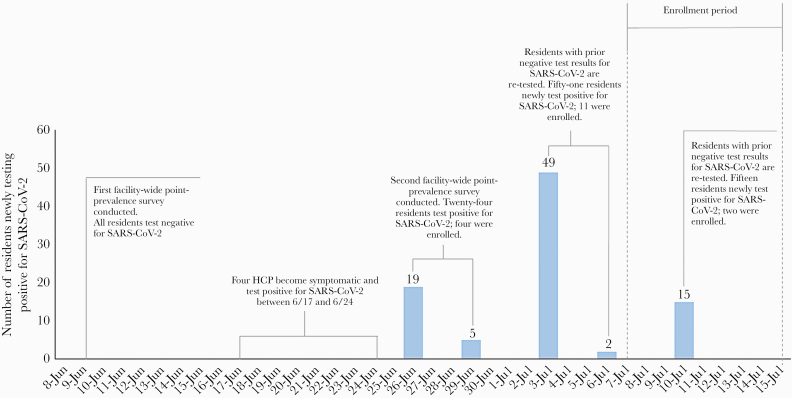
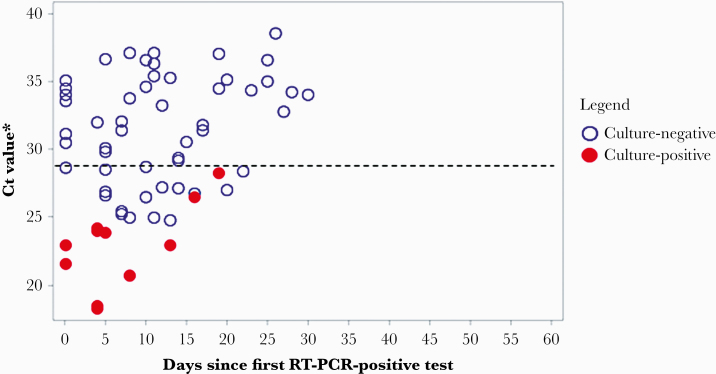
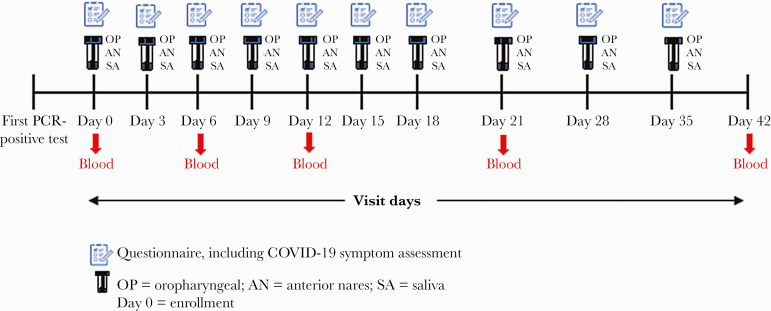
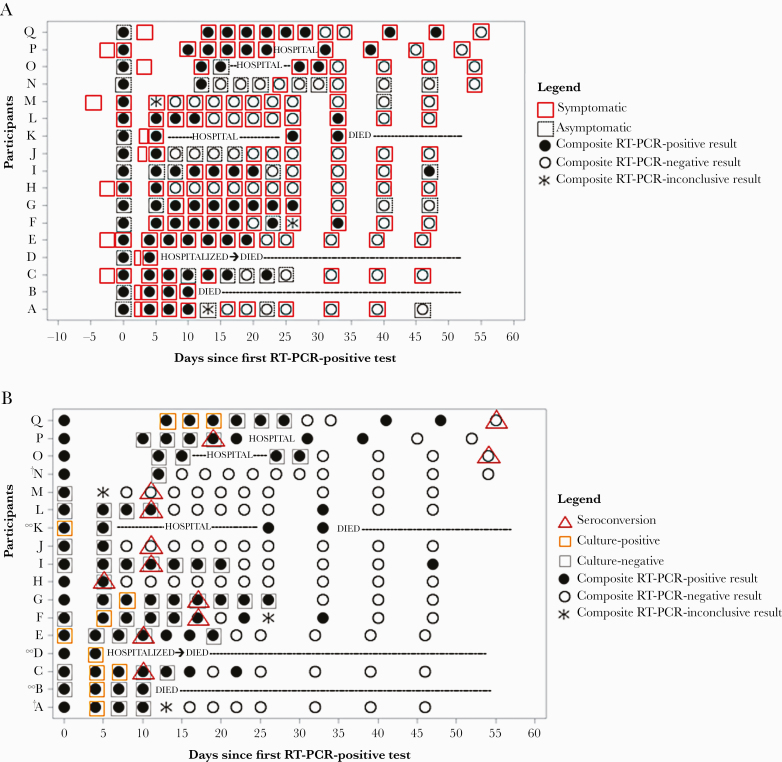
We enrolled residents within 15 days of their first positive SARS-CoV-2 test (diagnosis) at an Arkansas facility from July 7 to 15, 2020 and instead them for 42 days. Every 3 days for 21 days and then weekly, we assessed COVID-19 symptoms, collected specimens (oropharyngeal, anterior nares, and saliva), and reviewed medical charts. Blood for serology was collected on days 0, 6, 12, 21, and 42. Infectivity was defined by positive culture. Duration of culture positivity was compared with duration of COVID-19 symptoms and RT-PCR positivity. Data were summarized using measures of central tendency, frequencies, and proportions.
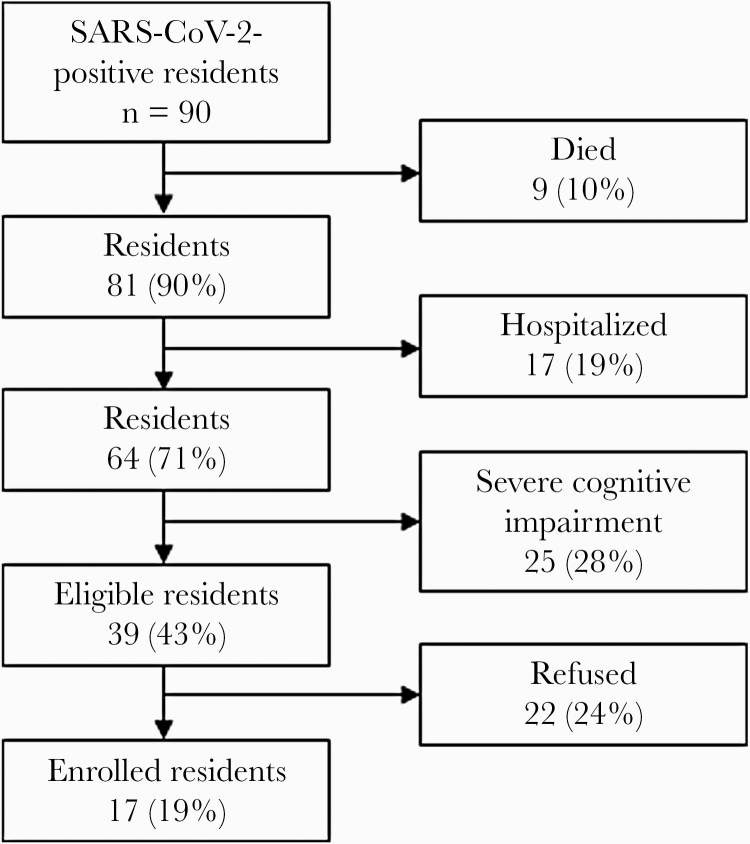
We enrolled 17 of 39 (44%) eligible residents. Median participant age was 82 years (range, 58-97 years). All had ≥3 underlying conditions. Median duration of RT-PCR positivity was 22 days (interquartile range [IQR], 8-31 days) from diagnosis; median duration of symptoms was 42 days (IQR, 28-49 days). Of 9 (53%) participants with any culture-positive specimens, 1 (11%) severely immunocompromised participant remained culture-positive 19 days from diagnosis; 8 of 9 (89%) were culture-positive ≤8 days from diagnosis. Seroconversion occurred in 12 of 12 (100%) surviving participants with ≥1 blood specimen; all participants were culture-negative before seroconversion.
Duration of infectivity was considerably shorter than duration of symptoms and RT-PCR positivity. Severe immunocompromise may prolong SARS-CoV-2 infectivity. Seroconversion indicated noninfectivity in this cohort.
为了评估患有基础疾病的老年人中严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的传染期,我们评估了养老院居民中2019冠状病毒病(COVID-19)症状的持续时间、逆转录聚合酶链反应(RT-PCR)阳性率和培养阳性率。
我们在2020年7月7日至15日期间,招募了阿肯色州一家机构中首次SARS-CoV-2检测呈阳性(确诊)后15天内的居民,并对他们进行了42天的随访。在21天内每3天进行一次,之后每周进行一次,我们评估COVID-19症状,采集标本(口咽、前鼻孔和唾液),并查阅病历。在第0、6、12、21和42天采集用于血清学检测的血液。传染性通过培养阳性来定义。将培养阳性的持续时间与COVID-19症状的持续时间和RT-PCR阳性率进行比较。数据使用集中趋势、频率和比例进行汇总。
我们招募了39名符合条件居民中的17名(44%)。参与者的年龄中位数为82岁(范围为58 - 97岁)。所有人都有≥3种基础疾病。从诊断开始,RT-PCR阳性的中位数持续时间为22天(四分位间距[IQR],8 - 31天);症状的中位数持续时间为42天(IQR,28 - 49天)。在9名(53%)有任何培养阳性标本的参与者中,1名(11%)严重免疫功能低下的参与者从诊断开始19天仍培养阳性;9名中的8名(89%)在诊断后≤8天培养阳性。12名有≥1份血液标本的存活参与者中有12名(100%)发生了血清转化;所有参与者在血清转化前培养均为阴性。
传染期的持续时间明显短于症状持续时间和RT-PCR阳性持续时间。严重免疫功能低下可能会延长SARS-CoV-2的传染性。血清转化表明该队列中的个体无传染性。