Institute of Virology, Faculty of Medicine and Medical Center, University of Freiburg, Freiburg, Germany.
Department of Anaesthesiology, Intensive Care, Emergency and Pain Medicine, University Hospital Wuerzburg, Wuerzburg, Germany.
Rev Med Virol. 2022 Sep;32(5):e2342. doi: 10.1002/rmv.2342. Epub 2022 Apr 2.
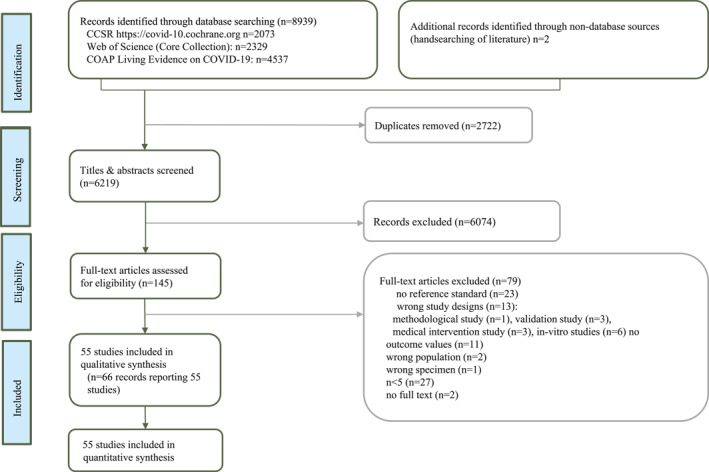
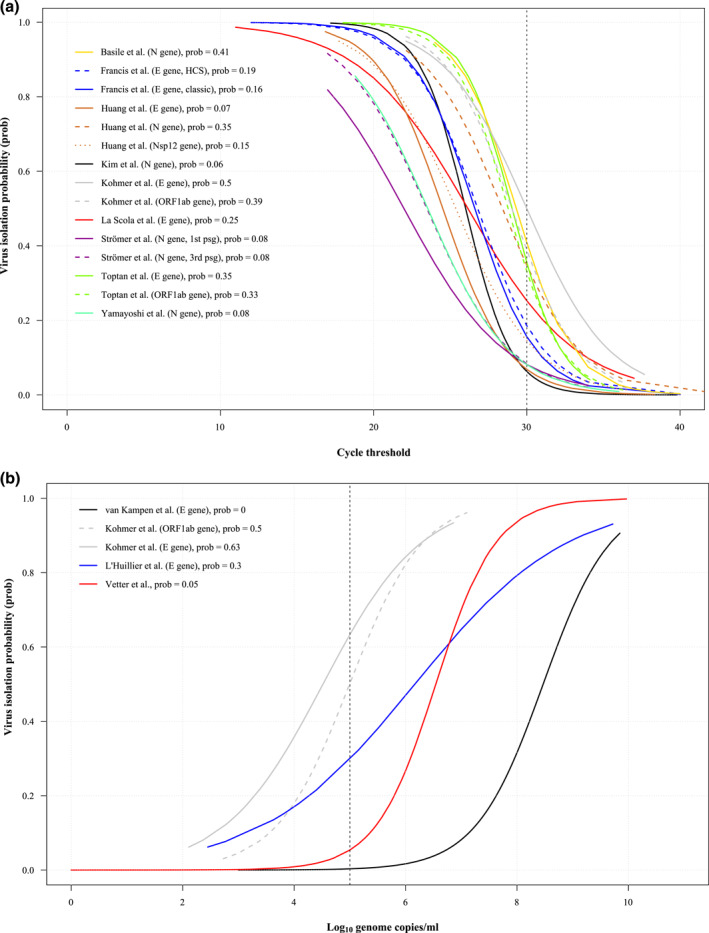
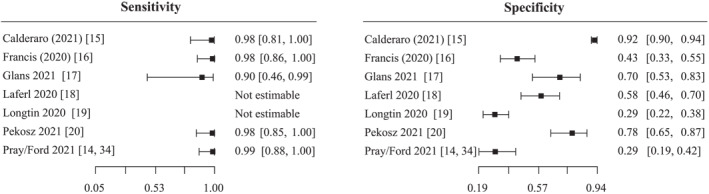
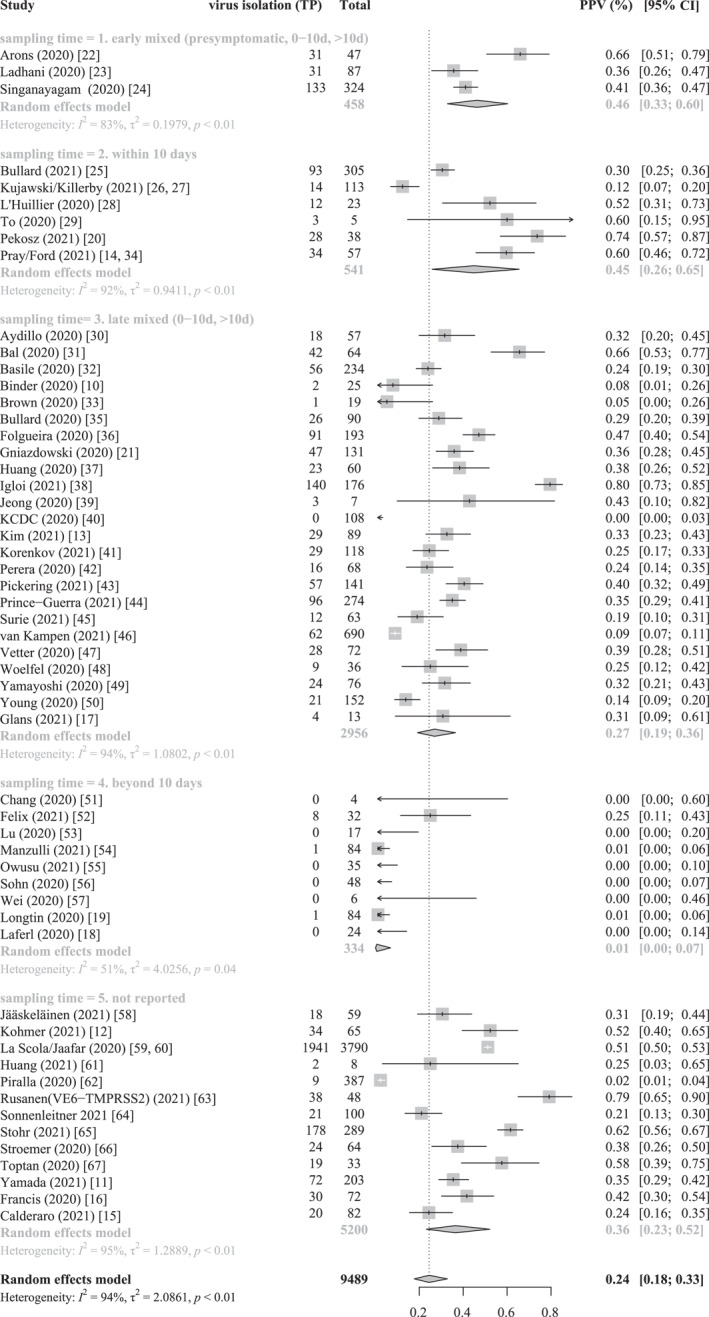
The cornerstone of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) detection is reverse-transcription polymerase chain reaction (RT-PCR) of viral RNA. As a surrogate assay SARS-CoV-2 RNA detection does not necessarily imply infectivity. Only virus isolation in permissive cell culture systems can indicate infectivity. Here, we review the evidence on RT-PCR performance in detecting infectious SARS-CoV-2. We searched for any studies that used RT-PCR and cell culture to determine infectious SARS-CoV-2 in respiratory samples. We assessed (i) diagnostic accuracy of RT-PCR compared to cell culture as reference test, (ii) performed meta-analysis of positive predictive values (PPV) and (iii) determined the virus isolation probabilities depending on cycle threshold (Ct) or log genome copies/ml using logistic regression. We included 55 studies. There is substantial statistical and clinical heterogeneity. Seven studies were included for diagnostic accuracy. Sensitivity ranged from 90% to 99% and specificity from 29% to 92%. In meta-analysis, the PPVs varied across subgroups with different sampling times after symptom onset, with 1% (95% confidence interval [CI], 0%-7%) in sampling beyond 10 days and 27% (CI, 19%-36%) to 46% (CI, 33%-60%) in subgroups that also included earlier samples. Estimates of virus isolation probability varied between 6% (CI, 0%-100%) and 50% (CI, 0%-100%) at a Ct value of 30 and between 0% (CI, 0%-22%) and 63% (CI, 0%-100%) at 5 log genome copies/ml. Evidence on RT-PCR performance in detecting infectious SARS-CoV-2 in respiratory samples was limited. Major limitations were heterogeneity and poor reporting. RT-PCR and cell culture protocols need further standardisation.
严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)检测的基础是病毒 RNA 的逆转录聚合酶链反应 (RT-PCR)。作为替代检测方法,SARS-CoV-2 RNA 检测不一定意味着具有传染性。只有在允许的细胞培养系统中分离病毒才能表明具有传染性。在这里,我们回顾了 RT-PCR 在检测传染性 SARS-CoV-2 方面的性能证据。我们搜索了任何使用 RT-PCR 和细胞培养来确定呼吸道样本中传染性 SARS-CoV-2 的研究。我们评估了 (i) RT-PCR 与细胞培养作为参考检测的诊断准确性,(ii) 对阳性预测值 (PPV) 进行荟萃分析,以及 (iii) 使用逻辑回归确定取决于循环阈值 (Ct) 或对数基因组拷贝/ml 的病毒分离概率。我们纳入了 55 项研究。存在大量统计学和临床异质性。有 7 项研究纳入了诊断准确性分析。灵敏度范围为 90%至 99%,特异性为 29%至 92%。荟萃分析中,不同亚组的 PPV 存在差异,症状出现后采样时间不同,采样时间超过 10 天的亚组为 1% (95%置信区间 [CI],0%-7%),同时包含更早采样的亚组为 27% (CI,19%-36%)至 46% (CI,33%-60%)。Ct 值为 30 时,病毒分离概率估计值在 6% (CI,0%-100%)和 50% (CI,0%-100%)之间,而在 5 对数基因组拷贝/ml 时,病毒分离概率估计值在 0% (CI,0%-22%)和 63% (CI,0%-100%)之间。关于 RT-PCR 在呼吸道样本中检测传染性 SARS-CoV-2 的性能的证据有限。主要限制是异质性和报告不佳。RT-PCR 和细胞培养方案需要进一步标准化。