From the South African Medical Research Council Vaccines and Infectious Diseases Analytics Research Unit (S.A.M., V.B., A.L.K., G.K., S.B., J.P., A.J., M.L., S.M., A.M., C.T., A.T., A.I.), African Leadership in Vaccinology Expertise (C.L.C.), Wits Reproductive Health and HIV Institute (L.F., E.H., M. Masenya, F.P., S.E.), the Antibody Immunity Research Unit, School of Pathology (J.N.B., C.K.W., P.L.M.), and the Perinatal HIV Research Unit (C.B.), Faculty of Health Sciences, and the Department of Science and Innovation/National Research Foundation South African Research Chair Initiative in Vaccine Preventable Diseases Unit (S.A.M., V.B., A.L.K., G.K., S.B., A.I.), University of the Witwatersrand, and the National Institute for Communicable Diseases (NICD) of the National Health Laboratory Service (NHLS) (J.N.B., C.K.W., P.L.M.), Johannesburg, Setshaba Research Centre, Tshwane (S.D.P., K.A., M. Malahleha, M. Masilela, K.M.), the Division of Pulmonology, Groote Schuur Hospital and the University of Cape Town (K.D., A.E., S.O.), and the Family Centre for Research with Ubuntu, Department of Paediatrics, University of Stellenbosch (S.L.B., M.G., L.R.), Cape Town, Soweto Clinical Trials Centre, Soweto (Q.E.B., A.E.B.), and the Africa Health Research Institute (S.-H.H., H.R., A.S.) and the KwaZulu-Natal Research and Innovation Sequencing Platform (KRISP), University of KwaZulu-Natal (S.P., H.T., T.O., A.S.), Durban - all in South Africa; the Oxford Vaccine Group, Department of Paediatrics (M.V., P.A., S.R., A.J.P.), and Jenner Institute, Nuffield Department of Medicine (T.L., S.G.), University of Oxford, Oxford, the Faculty of Infectious and Tropical Diseases, Department of Immunology and Infection, London School of Hygiene and Tropical Medicine, London (K.D., A.E.), Division of Infection and Immunity, University College London, London (K.D.), and AstraZeneca Biopharmaceuticals, Cambridge (N.M.D., E.J.K., T.L.V.) - all in the United Kingdom; and Max Planck Institute for Infection Biology, Berlin (S.-H.H., H.R.).
N Engl J Med. 2021 May 20;384(20):1885-1898. doi: 10.1056/NEJMoa2102214. Epub 2021 Mar 16.
Assessment of the safety and efficacy of vaccines against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in different populations is essential, as is investigation of the efficacy of the vaccines against emerging SARS-CoV-2 variants of concern, including the B.1.351 (501Y.V2) variant first identified in South Africa.
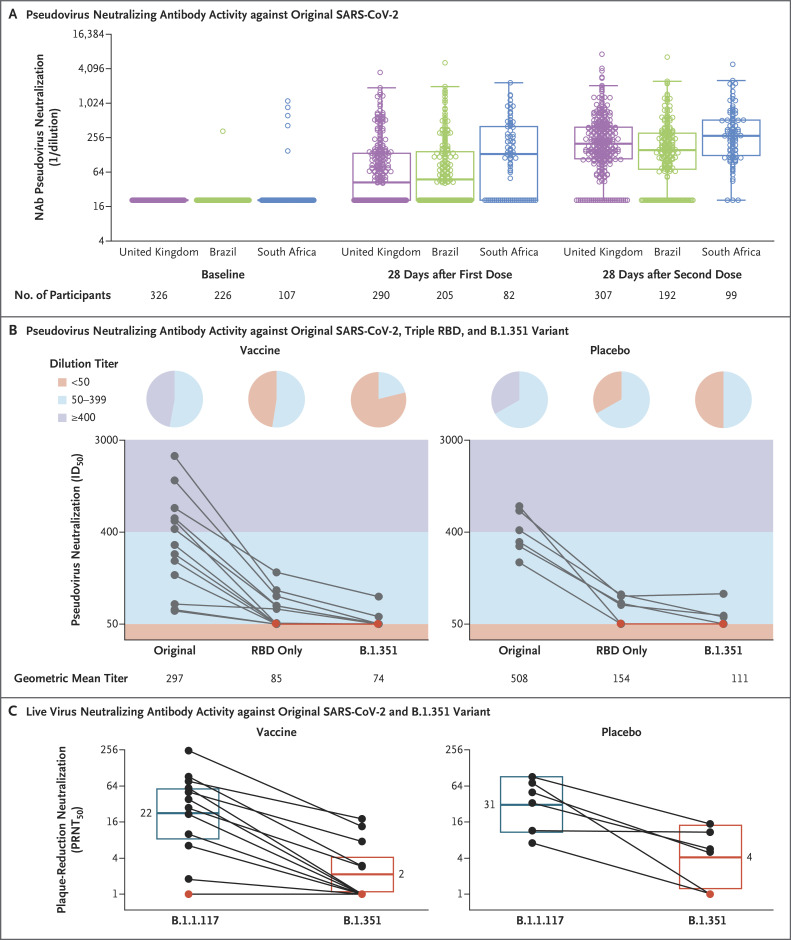
We conducted a multicenter, double-blind, randomized, controlled trial to assess the safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) in people not infected with the human immunodeficiency virus (HIV) in South Africa. Participants 18 to less than 65 years of age were assigned in a 1:1 ratio to receive two doses of vaccine containing 5×10 viral particles or placebo (0.9% sodium chloride solution) 21 to 35 days apart. Serum samples obtained from 25 participants after the second dose were tested by pseudovirus and live-virus neutralization assays against the original D614G virus and the B.1.351 variant. The primary end points were safety and efficacy of the vaccine against laboratory-confirmed symptomatic coronavirus 2019 illness (Covid-19) more than 14 days after the second dose.
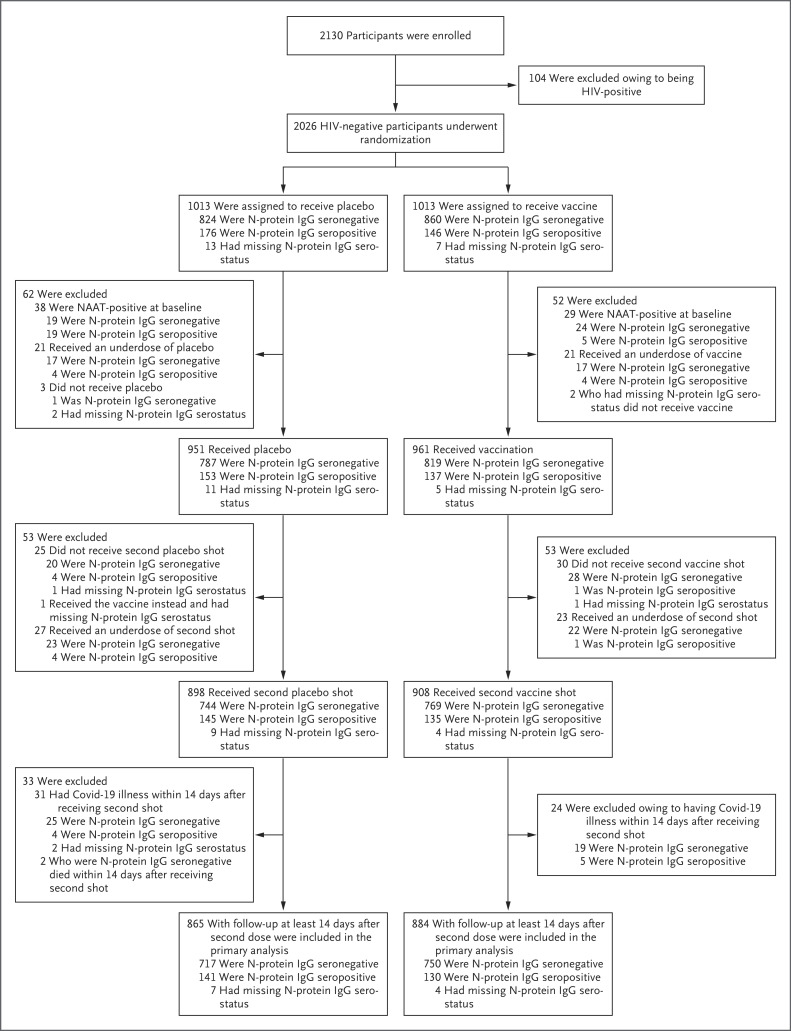
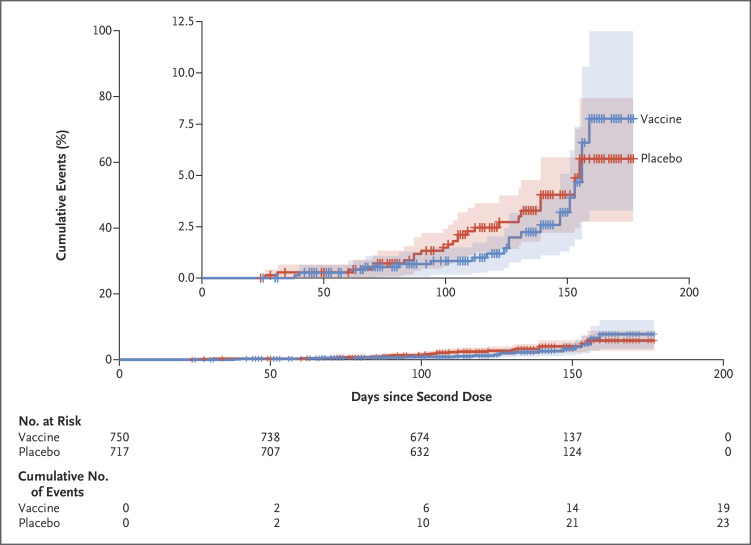
Between June 24 and November 9, 2020, we enrolled 2026 HIV-negative adults (median age, 30 years); 1010 and 1011 participants received at least one dose of placebo or vaccine, respectively. Both the pseudovirus and the live-virus neutralization assays showed greater resistance to the B.1.351 variant in serum samples obtained from vaccine recipients than in samples from placebo recipients. In the primary end-point analysis, mild-to-moderate Covid-19 developed in 23 of 717 placebo recipients (3.2%) and in 19 of 750 vaccine recipients (2.5%), for an efficacy of 21.9% (95% confidence interval [CI], -49.9 to 59.8). Among the 42 participants with Covid-19, 39 cases (95.1% of 41 with sequencing data) were caused by the B.1.351 variant; vaccine efficacy against this variant, analyzed as a secondary end point, was 10.4% (95% CI, -76.8 to 54.8). The incidence of serious adverse events was balanced between the vaccine and placebo groups.
A two-dose regimen of the ChAdOx1 nCoV-19 vaccine did not show protection against mild-to-moderate Covid-19 due to the B.1.351 variant. (Funded by the Bill and Melinda Gates Foundation and others; ClinicalTrials.gov number, NCT04444674; Pan African Clinical Trials Registry number, PACTR202006922165132).
评估针对严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)的疫苗在不同人群中的安全性和有效性至关重要,同时还需要调查疫苗对包括首先在南非发现的 B.1.351(501Y.V2)变体在内的新兴 SARS-CoV-2 关切变体的有效性。
我们进行了一项多中心、双盲、随机、对照试验,以评估在南非未感染人类免疫缺陷病毒(HIV)的人群中 ChAdOx1 nCoV-19 疫苗(AZD1222)的安全性和有效性。18 岁以下至 65 岁以下的参与者按照 1:1 的比例随机分配,接受两剂含有 5×10 个病毒颗粒的疫苗或安慰剂(0.9%氯化钠溶液),间隔 21 至 35 天。在第二次给药后,从 25 名参与者中获得的血清样本通过假病毒和活病毒中和测定法针对原始 D614G 病毒和 B.1.351 变体进行了测试。主要终点是第二次给药后 14 天以上,疫苗对实验室确诊的有症状 2019 年冠状病毒病(Covid-19)的安全性和有效性。
2020 年 6 月 24 日至 11 月 9 日期间,我们招募了 2026 名 HIV 阴性成年人(中位年龄 30 岁);分别有 1010 名和 1011 名参与者至少接受了一剂安慰剂或疫苗。在接受疫苗的参与者的血清样本中,假病毒和活病毒中和测定法均显示出对 B.1.351 变体的更大抵抗力,而在接受安慰剂的参与者的血清样本中则没有。在主要终点分析中,717 名安慰剂接受者中有 23 名(3.2%)和 750 名疫苗接受者中有 19 名(2.5%)出现轻度至中度 Covid-19,疫苗效力为 21.9%(95%置信区间[CI],-49.9 至 59.8)。在 42 名患有 Covid-19 的参与者中,有 39 例(41 例有测序数据的 95.1%)由 B.1.351 变体引起;作为次要终点分析的针对该变体的疫苗效力为 10.4%(95%CI,-76.8 至 54.8)。疫苗和安慰剂组之间严重不良事件的发生率是平衡的。
两剂 ChAdOx1 nCoV-19 疫苗方案并未显示出对由 B.1.351 变体引起的轻度至中度 Covid-19 的保护作用。(由比尔及梅琳达·盖茨基金会和其他机构资助;ClinicalTrials.gov 编号,NCT04444674;泛非临床试验注册处编号,PACTR202006922165132)。