Oxford Vaccine Group, Department of Paediatrics, University of Oxford, Oxford, UK.
Big Data Institute, Nuffield Department of Medicine, University of Oxford, Oxford, UK.
Lancet. 2021 Apr 10;397(10282):1351-1362. doi: 10.1016/S0140-6736(21)00628-0. Epub 2021 Mar 30.
A new variant of SARS-CoV-2, B.1.1.7, emerged as the dominant cause of COVID-19 disease in the UK from November, 2020. We report a post-hoc analysis of the efficacy of the adenoviral vector vaccine, ChAdOx1 nCoV-19 (AZD1222), against this variant.
Volunteers (aged ≥18 years) who were enrolled in phase 2/3 vaccine efficacy studies in the UK, and who were randomly assigned (1:1) to receive ChAdOx1 nCoV-19 or a meningococcal conjugate control (MenACWY) vaccine, provided upper airway swabs on a weekly basis and also if they developed symptoms of COVID-19 disease (a cough, a fever of 37·8°C or higher, shortness of breath, anosmia, or ageusia). Swabs were tested by nucleic acid amplification test (NAAT) for SARS-CoV-2 and positive samples were sequenced through the COVID-19 Genomics UK consortium. Neutralising antibody responses were measured using a live-virus microneutralisation assay against the B.1.1.7 lineage and a canonical non-B.1.1.7 lineage (Victoria). The efficacy analysis included symptomatic COVID-19 in seronegative participants with a NAAT positive swab more than 14 days after a second dose of vaccine. Participants were analysed according to vaccine received. Vaccine efficacy was calculated as 1 - relative risk (ChAdOx1 nCoV-19 vs MenACWY groups) derived from a robust Poisson regression model. This study is continuing and is registered with ClinicalTrials.gov, NCT04400838, and ISRCTN, 15281137.
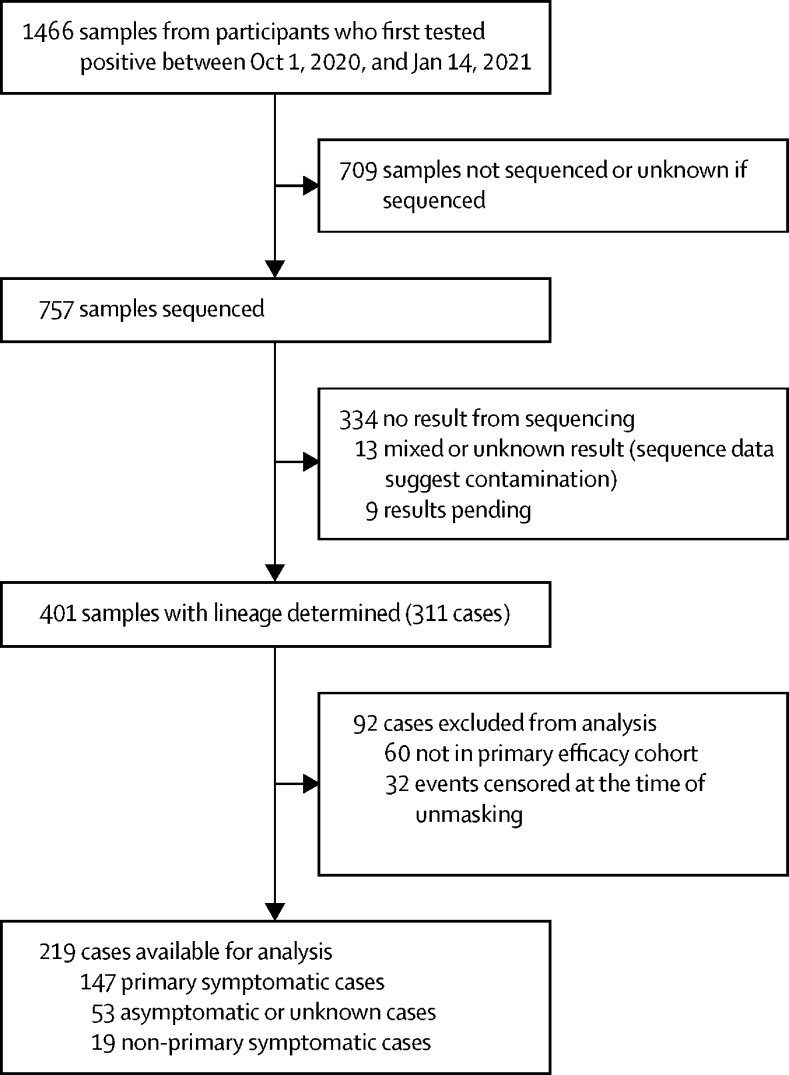
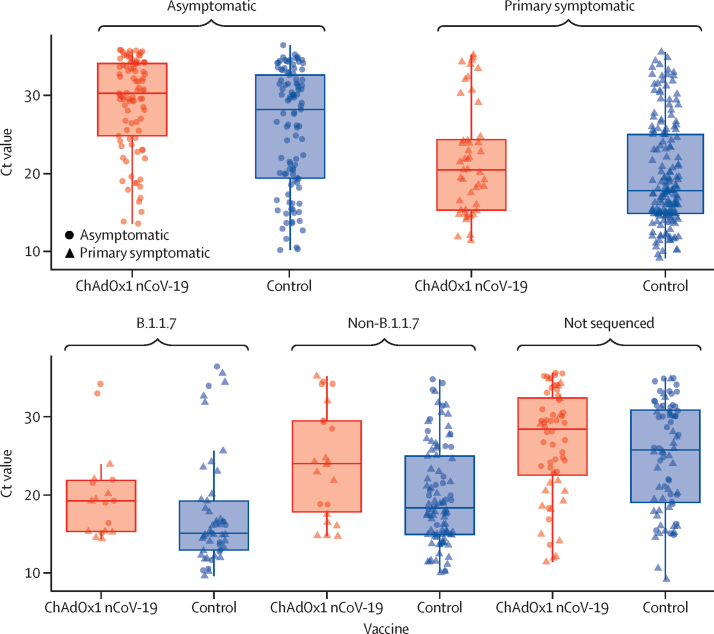
Participants in efficacy cohorts were recruited between May 31 and Nov 13, 2020, and received booster doses between Aug 3 and Dec 30, 2020. Of 8534 participants in the primary efficacy cohort, 6636 (78%) were aged 18-55 years and 5065 (59%) were female. Between Oct 1, 2020, and Jan 14, 2021, 520 participants developed SARS-CoV-2 infection. 1466 NAAT positive nose and throat swabs were collected from these participants during the trial. Of these, 401 swabs from 311 participants were successfully sequenced. Laboratory virus neutralisation activity by vaccine-induced antibodies was lower against the B.1.1.7 variant than against the Victoria lineage (geometric mean ratio 8·9, 95% CI 7·2-11·0). Clinical vaccine efficacy against symptomatic NAAT positive infection was 70·4% (95% CI 43·6-84·5) for B.1.1.7 and 81·5% (67·9-89·4) for non-B.1.1.7 lineages.
ChAdOx1 nCoV-19 showed reduced neutralisation activity against the B.1.1.7 variant compared with a non-B.1.1.7 variant in vitro, but the vaccine showed efficacy against the B.1.1.7 variant of SARS-CoV-2.
UK Research and Innovation, National Institute for Health Research (NIHR), Coalition for Epidemic Preparedness Innovations, NIHR Oxford Biomedical Research Centre, Thames Valley and South Midlands NIHR Clinical Research Network, and AstraZeneca.
一种新的 SARS-CoV-2 变体 B.1.1.7 自 2020 年 11 月起成为英国 COVID-19 疾病的主要病因。我们报告了腺病毒载体疫苗 ChAdOx1 nCoV-19(AZD1222)对这种变体的疗效的事后分析。
在英国参加 2/3 期疫苗功效研究的志愿者(年龄≥18 岁),以 1:1 的比例随机分配(随机分组)接受 ChAdOx1 nCoV-19 或脑膜炎球菌结合疫苗(MenACWY),每周提供上呼吸道拭子,如果出现 COVID-19 疾病的症状(咳嗽、37.8°C 或更高的发热、呼吸急促、嗅觉丧失或味觉丧失)也提供拭子。拭子通过核酸扩增试验(NAAT)进行 SARS-CoV-2 检测,如果为阳性,则通过 COVID-19 基因组英国联盟进行测序。使用针对 B.1.1.7 谱系和非 B.1.1.7 谱系(维多利亚)的活病毒微量中和测定法测量中和抗体反应。疗效分析包括血清学阴性参与者在第二剂疫苗接种后 14 天以上的 NAAT 阳性拭子出现有症状的 COVID-19。参与者根据接受的疫苗进行分析。疫苗功效计算为 1-相对风险(ChAdOx1 nCoV-19 与 MenACWY 组),源自稳健的泊松回归模型。该研究正在进行中,并在 ClinicalTrials.gov、NCT04400838 和 ISRCTN、15281137 上注册。
功效队列的参与者于 2020 年 5 月 31 日至 11 月 13 日招募,并于 2020 年 8 月 3 日至 12 月 30 日接受了加强剂量。主要功效队列中的 8534 名参与者中,6636 名(78%)年龄在 18-55 岁之间,5065 名(59%)为女性。2020 年 10 月 1 日至 2021 年 1 月 14 日期间,520 名参与者感染了 SARS-CoV-2。在试验期间,从这些参与者中采集了 1466 份鼻喉 NAAT 阳性拭子。其中,401 份来自 311 名参与者的拭子成功测序。疫苗诱导的抗体对 B.1.1.7 变体的实验室病毒中和活性低于对维多利亚谱系的中和活性(几何平均比 8.9,95%CI 7.2-11.0)。针对有症状的 NAAT 阳性感染的临床疫苗功效为 B.1.1.7 为 70.4%(95%CI 43.6-84.5),非 B.1.1.7 谱系为 81.5%(67.9-89.4)。
ChAdOx1 nCoV-19 体外对 B.1.1.7 变体的中和活性降低,但该疫苗对 SARS-CoV-2 的 B.1.1.7 变体具有功效。
英国研究与创新、英国国家卫生研究院(NIHR)、流行病防范创新联盟、NIHR 牛津生物医学研究中心、泰晤士河谷和南米德兰 NIHR 临床研究网络以及阿斯利康。