Hasan Amal, Al-Ozairi Ebaa, Al-Baqsumi Zahraa, Ahmad Rasheed, Al-Mulla Fahd
Department of Immunology and Microbiology, Research Division, Dasman Diabetes Institute, Dasman, Kuwait City, Kuwait.
Clinical Research Unit, Medical Division, Dasman Diabetes Institute, Dasman, Kuwait City, Kuwait.
Immunotargets Ther. 2021 Mar 9;10:63-85. doi: 10.2147/ITT.S280706. eCollection 2021.
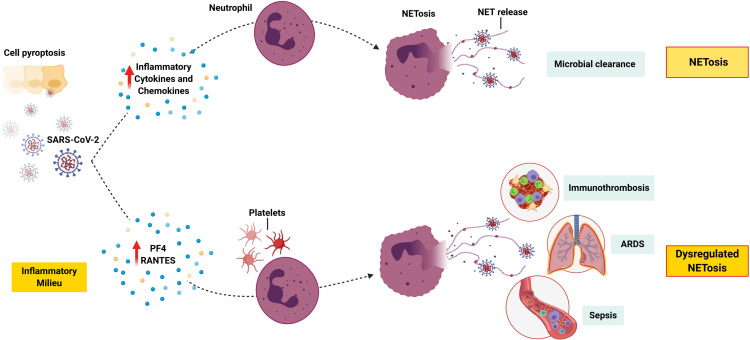
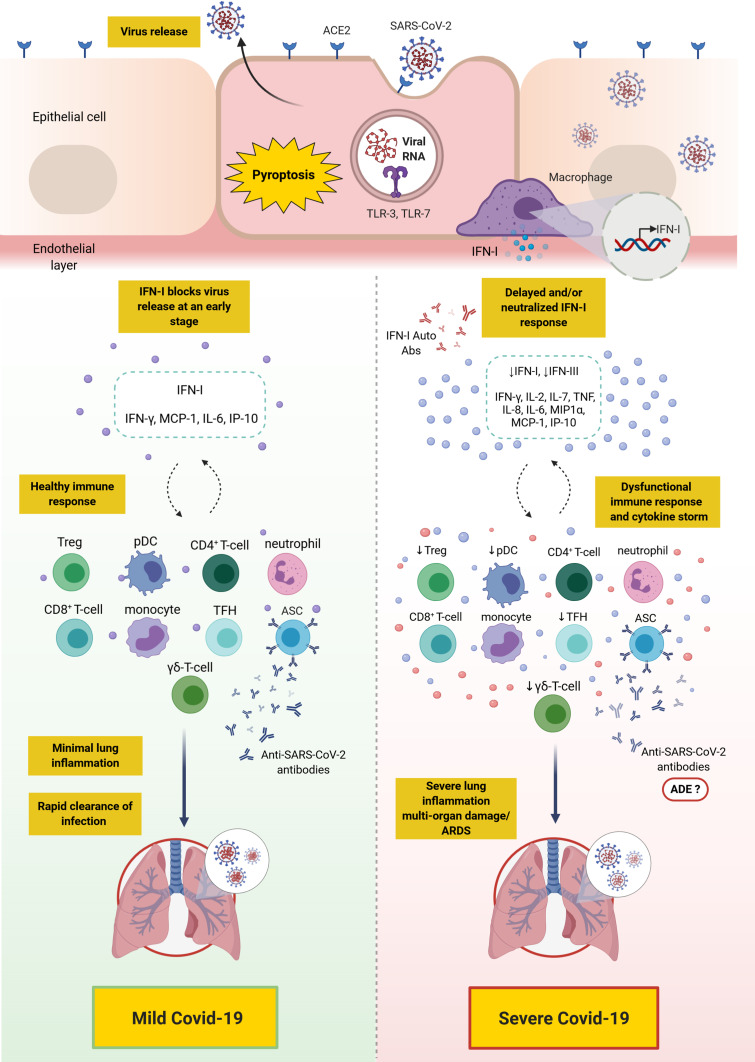
Coronavirus disease 2019 (Covid-19), caused by the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), can range in severity from asymptomatic to severe/critical disease. SARS-CoV-2 uses angiotensin-converting enzyme 2 to infect cells leading to a strong inflammatory response, which is most profound in patients who progress to severe Covid-19. Recent studies have begun to unravel some of the differences in the innate and adaptive immune response to SARS-CoV-2 in patients with different degrees of disease severity. These studies have attributed the severe form of Covid-19 to a dysfunctional innate immune response, such as a delayed and/or deficient type I interferon response, coupled with an exaggerated and/or a dysfunctional adaptive immunity. Differences in T-cell (including CD4 T-cells, CD8 T-cells, T follicular helper cells, γδ-T-cells, and regulatory T-cells) and B-cell (transitional cells, double-negative 2 cells, antibody-secreting cells) responses have been identified in patients with severe disease compared to mild cases. Moreover, differences in the kinetic/titer of neutralizing antibody responses have been described in severe disease, which may be confounded by antibody-dependent enhancement. Importantly, the presence of preexisting autoantibodies against type I interferon has been described as a major cause of severe/critical disease. Additionally, priorVaccine and multiple vaccine exposure, trained innate immunity, cross-reactive immunity, and serological immune imprinting may all contribute towards disease severity and outcome. Several therapeutic and preventative approaches have been under intense investigations; these include vaccines (three of which have passed Phase 3 clinical trials), therapeutic antibodies, and immunosuppressants.
2019冠状病毒病(Covid-19)由新型冠状病毒严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引起,其严重程度可从无症状到重症/危重症。SARS-CoV-2利用血管紧张素转换酶2感染细胞,导致强烈的炎症反应,这在进展为重症Covid-19的患者中最为明显。最近的研究已开始揭示不同疾病严重程度的患者对SARS-CoV-2的先天性和适应性免疫反应的一些差异。这些研究将重症Covid-19的严重形式归因于先天性免疫反应功能失调,例如I型干扰素反应延迟和/或不足,同时伴有适应性免疫反应过度和/或功能失调。与轻症病例相比,重症患者的T细胞(包括CD4 T细胞、CD8 T细胞、滤泡辅助性T细胞、γδ-T细胞和调节性T细胞)和B细胞(过渡细胞、双阴性2细胞、抗体分泌细胞)反应存在差异。此外,重症患者的中和抗体反应动力学/滴度也存在差异,这可能因抗体依赖性增强而混淆。重要的是,针对I型干扰素的预先存在的自身抗体的存在被认为是重症/危重症疾病的主要原因。此外,既往疫苗接种和多次疫苗暴露、训练有素的先天性免疫、交叉反应性免疫和血清学免疫印记都可能影响疾病的严重程度和转归。目前正在对几种治疗和预防方法进行深入研究;这些方法包括疫苗(其中三种已通过3期临床试验)、治疗性抗体和免疫抑制剂。