Clinical Epidemiology Unit, Department of Clinical Sciences Lund, Orthopaedics, Lund University, Skåne University Hospital, Remissgatan 4, SE-221 85, Lund, Sweden.
Centre for Economic Demography, Lund University, Lund, Sweden.
BMC Public Health. 2021 Mar 17;21(1):519. doi: 10.1186/s12889-021-10567-5.
Avoidable mortality is considered as a potential indicator of the influences of public health policies and healthcare quality on population health. This study aimed to examine the trend in avoidable mortality and its influence on rising life expectancy (LE) and declining gender gap in LE (GGLE) in Sweden.
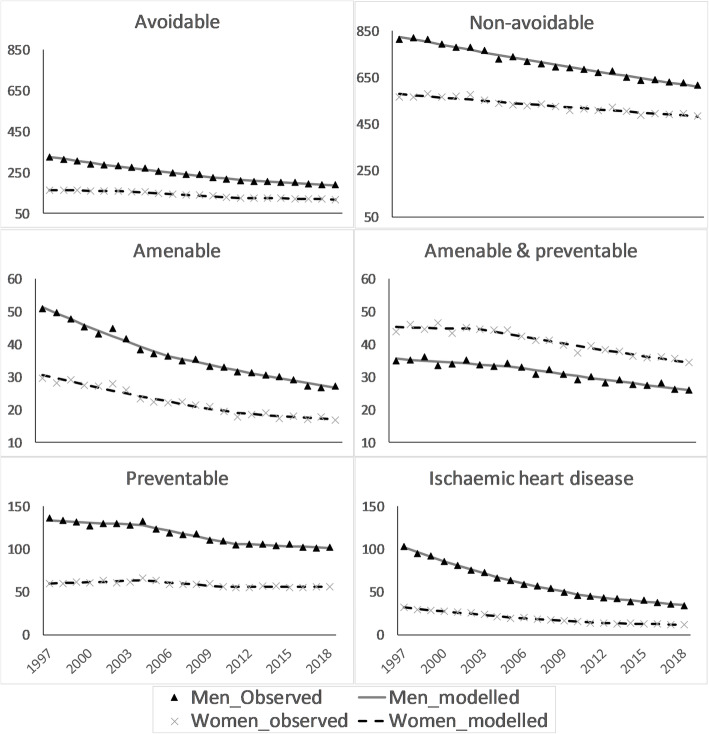
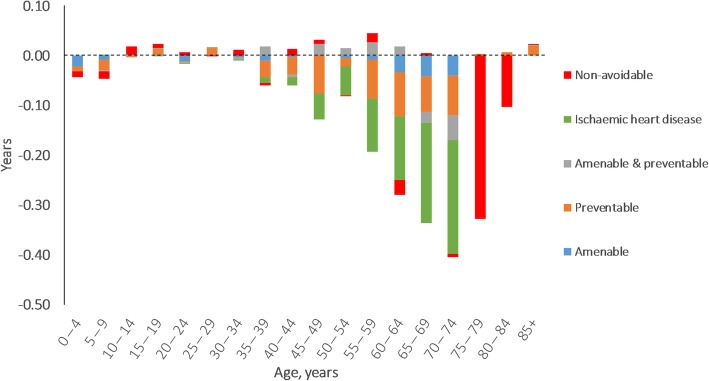
We extracted data on causes of death by age, sex, and year from national registry from 1997 to 2018. The UK Office for National Statistics definition was used to divide causes of death into five mutually exclusive categories: amenable, preventable, amenable & preventable, ischemic heart disease (IHD), and non-avoidable causes. We applied Joinpoint regression to analyse temporal trends in age-standardized mortality rates. The Arriaga method was applied to decompose changes in LE and GGLE by age group and causes of death.
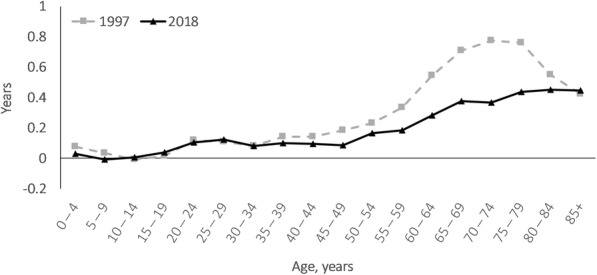
Average annual reductions in avoidable vs. non-avoidable mortality were 2.6% (95% CI:2.5, 2.7) vs. 1.4% (95% CI:1.3, 1.5) in men, and 1.6% (95% CI:1.4, 1.9) vs. 0.9% (95% CI:0.7, 1.0) in women over the study period. LE in men rose by 4.1 years between 1997 and 2018 (from 72.8 to 76.9 years), of which 2.4 years (59.3%) were attributable to reductions in avoidable mortality. Corresponding LE gain was 2.3 years in women (from 78.0 in 1997 to 80.3 in 2018) and avoidable mortality accounted for 1.0 year (45.6%) of this gain. Between 1997 and 2018, the GGLE narrowed by 1.9 years, of which 1.4 years (77.7%) were attributable to avoidable causes. Among avoidable causes, while preventable causes had the largest contribution to the GGLE, IHD had the greatest contributions to LE gains and the narrowing GGLE.
Our findings showed that avoidable causes had a substantial contribution to gain in LE with more profound gain in men than in women, resulting in narrowing the GGLE. Lower pace of reductions in preventable than amenable mortality highlights the need for improving the effectiveness of inter-sectoral health policies aimed at behavioural changes.
可避免死亡率被认为是公共卫生政策和医疗质量对人口健康影响的潜在指标。本研究旨在探讨瑞典可避免死亡率的趋势及其对预期寿命(LE)上升和 LE 性别差距缩小(GGLE)的影响。
我们从 1997 年至 2018 年的国家登记处提取了按年龄、性别和年份划分的死因数据。采用英国国家统计局的定义将死因分为五个互斥类别:可治疗、可预防、可治疗和预防、缺血性心脏病(IHD)和不可避免的死因。我们应用 Joinpoint 回归分析了年龄标准化死亡率的时间趋势。应用 Arriaga 方法按年龄组和死因分解 LE 和 GGLE 的变化。
在研究期间,男性中可避免与不可避免死亡率的平均年降幅分别为 2.6%(95%CI:2.5,2.7)和 1.4%(95%CI:1.3,1.5),女性分别为 1.6%(95%CI:1.4,1.9)和 0.9%(95%CI:0.7,1.0)。男性的 LE 在 1997 年至 2018 年间增加了 4.1 年(从 72.8 年增加到 76.9 年),其中 2.4 年(59.3%)归因于可避免死亡率的降低。女性相应的 LE 增加了 2.3 年(从 1997 年的 78.0 年增加到 2018 年的 80.3 年),其中可避免死亡率占 1.0 年(45.6%)。1997 年至 2018 年间,GGLE 缩小了 1.9 年,其中 1.4 年(77.7%)归因于可避免的原因。在可避免的原因中,虽然可预防的原因对 GGLE 的贡献最大,但 IHD 对 LE 增加和 GGLE 缩小的贡献最大。
我们的研究结果表明,可避免的原因对 LE 的增加有很大的贡献,男性的增加幅度大于女性,导致 GGLE 缩小。预防死亡率的降低速度低于可治疗死亡率,这突出表明需要提高旨在改变行为的部门间卫生政策的有效性。