Jo Youngji, Jamieson Lise, Edoka Ijeoma, Long Lawrence, Silal Sheetal, Pulliam Juliet R C, Moultrie Harry, Sanne Ian, Meyer-Rath Gesine, Nichols Brooke E
Section of Infectious Disease, Department of Medicine, Boston Medical Center, Boston, Massachusetts, USA.
Health Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Open Forum Infect Dis. 2021 Jan 29;8(3):ofab040. doi: 10.1093/ofid/ofab040. eCollection 2021 Mar.
Dexamethasone and remdesivir have the potential to reduce coronavirus disease 2019 (COVID)-related mortality or recovery time, but their cost-effectiveness in countries with limited intensive care resources is unknown.
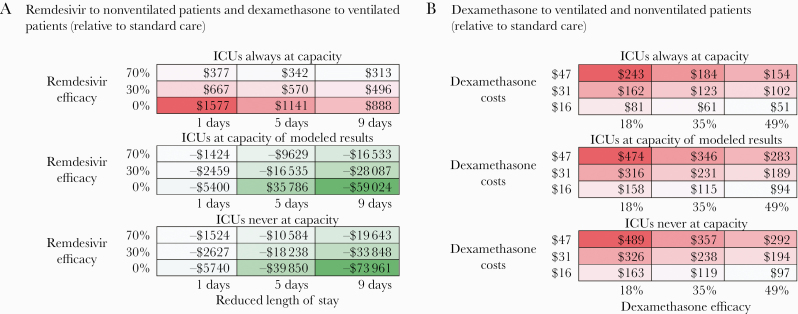
We projected intensive care unit (ICU) needs and capacity from August 2020 to January 2021 using the South African National COVID-19 Epi Model. We assessed the cost-effectiveness of (1) administration of dexamethasone to ventilated patients and remdesivir to nonventilated patients, (2) dexamethasone alone to both nonventilated and ventilated patients, (3) remdesivir to nonventilated patients only, and (4) dexamethasone to ventilated patients only, all relative to a scenario of standard care. We estimated costs from the health care system perspective in 2020 US dollars, deaths averted, and the incremental cost-effectiveness ratios of each scenario.
Remdesivir for nonventilated patients and dexamethasone for ventilated patients was estimated to result in 408 (uncertainty range, 229-1891) deaths averted (assuming no efficacy [uncertainty range, 0%-70%] of remdesivir) compared with standard care and to save $15 million. This result was driven by the efficacy of dexamethasone and the reduction of ICU-time required for patients treated with remdesivir. The scenario of dexamethasone alone for nonventilated and ventilated patients requires an additional $159 000 and averts 689 [uncertainty range, 330-1118] deaths, resulting in $231 per death averted, relative to standard care.
The use of remdesivir for nonventilated patients and dexamethasone for ventilated patients is likely to be cost-saving compared with standard care by reducing ICU days. Further efforts to improve recovery time with remdesivir and dexamethasone in ICUs could save lives and costs in South Africa.
地塞米松和瑞德西韦有可能降低2019冠状病毒病(COVID-19)相关死亡率或缩短康复时间,但在重症监护资源有限的国家,它们的成本效益尚不清楚。
我们使用南非国家COVID-19疫情模型预测了2020年8月至2021年1月期间的重症监护病房(ICU)需求和容量。我们评估了以下四种情况相对于标准治疗方案的成本效益:(1)对使用呼吸机的患者使用地塞米松,对未使用呼吸机的患者使用瑞德西韦;(2)对未使用呼吸机和使用呼吸机的患者均单独使用地塞米松;(3)仅对未使用呼吸机的患者使用瑞德西韦;(4)仅对使用呼吸机的患者使用地塞米松。我们从医疗保健系统的角度以2020年美元估算成本、避免的死亡人数以及每种情况的增量成本效益比。
与标准治疗相比,预计对未使用呼吸机的患者使用瑞德西韦、对使用呼吸机的患者使用地塞米松可避免408例(不确定范围为229 - 1891例)死亡(假设瑞德西韦无疗效[不确定范围为0% - 70%]),并节省1500万美元。这一结果得益于地塞米松的疗效以及使用瑞德西韦治疗的患者所需ICU时间的减少。相对于标准治疗,对未使用呼吸机和使用呼吸机的患者均单独使用地塞米松的方案需要额外花费15.9万美元,可避免689例(不确定范围为330 - 1118例)死亡,每避免一例死亡的成本为231美元。
与标准治疗相比,对未使用呼吸机的患者使用瑞德西韦、对使用呼吸机的患者使用地塞米松通过减少ICU天数可能节省成本。在ICU中进一步努力使用瑞德西韦和地塞米松来缩短康复时间,可在南非挽救生命并降低成本。