Wright Megan K, Gong Wu, Hart Kimberly, Self Wesley H, Ward Michael J
Vanderbilt University School of Medicine Nashville Tennessee USA.
Department of Biostatistics Vanderbilt University School of Medicine Nashville Tennessee USA.
J Am Coll Emerg Physicians Open. 2021 Mar 6;2(2):e12385. doi: 10.1002/emp2.12385. eCollection 2021 Apr.
Interfacility transfers between emergency department (EDs) are common and at times unnecessary. We sought to examine the role of health insurance status with potentially avoidable transfers.
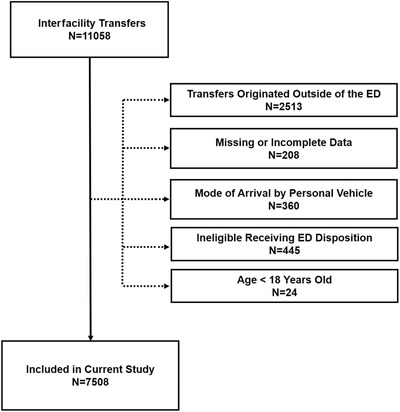
We conducted a retrospective observational analysis using hospital electronic administrative data of all interfacility ED-to-ED transfers to a single, quaternary care adult ED in 2018. We defined a potentially avoidable transfer as an ED-to-ED transfer in which the patient did not receive a procedure from a specialist at the receiving hospital and was discharged from the ED or the receiving hospital within 24 hours of arrival. We constructed a multivariable logistic regression model to examine whether insurance status was associated with potentially avoidable transfers among all ED-to-ED transfers adjusting for patient demographics, severity, mode of arrival, clinical condition, and rurality.
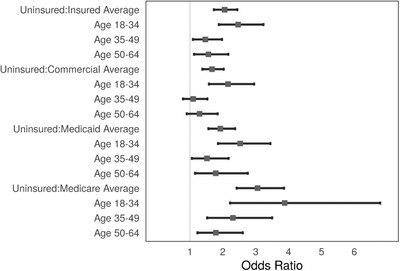
Among 7508 transfers, 1862 (25%) were potentially avoidable and were more likely to be uninsured (20% vs 9%). In the multivariable analysis, among ED-to-ED transfers for adults aged 18-64 years old who were uninsured (vs any insurance) were significantly more likely to be potentially avoidable (adjusted odds ratio [aOR] 2.1 [1.7, 2.4]) and there is a significant interaction with age. Potentially avoidable transfers increased with younger age, male sex, black (vs white), small rural classification (vs urban), and arrival by ground ambulance (vs flight).
Potentially avoidable transfers comprised 1 in 4 transfers. Patients who lack insurance were more than twice as likely to be classified as potentially avoidable even after evaluating for confounders and interactions. This effect was most pronounced among younger patients. Further research is needed to explore why uninsured patients are disproportionately more likely to experience potentially avoidable transfers.
急诊科(ED)之间的机构间转运很常见,有时甚至不必要。我们试图研究医疗保险状况在潜在可避免转运中所起的作用。
我们利用2018年所有从一个急诊科到另一个单一的四级成人急诊科的机构间转运的医院电子管理数据进行了一项回顾性观察分析。我们将潜在可避免转运定义为患者在接收医院未接受专科医生的诊疗且在到达后24小时内从急诊科或接收医院出院的急诊科之间的转运。我们构建了一个多变量逻辑回归模型,以检验在调整患者人口统计学、严重程度、到达方式、临床状况和农村地区因素后,保险状况是否与所有急诊科之间的转运中潜在可避免的转运相关。
在7508次转运中,1862次(25%)是潜在可避免的,且这些患者更有可能未参保(20%对9%)。在多变量分析中,对于18 - 64岁未参保(与任何参保情况相比)的成人急诊科之间的转运,潜在可避免的可能性显著更高(调整后的优势比[aOR]为2.1[1.7, 2.4]),并且与年龄存在显著交互作用。潜在可避免的转运随着年龄较小、男性、黑人(与白人相比)、农村小分类(与城市相比)以及通过地面救护车到达(与空中转运相比)而增加。
潜在可避免的转运占所有转运的四分之一。即使在评估了混杂因素和交互作用之后,未参保患者被归类为潜在可避免的可能性也高出两倍多。这种影响在年轻患者中最为明显。需要进一步研究以探索未参保患者更易经历潜在可避免转运的原因。