Clarke-Deelder Emma, Suharlim Christian, Chatterjee Susmita, Brenzel Logan, Ray Arindam, Cohen Jessica L, McConnell Margaret, Resch Stephen C, Menzies Nicolas A
Department of Global Health and Population, Harvard T. H. Chan School of Public Health, 665 Huntington Avenue, Boston, MA 02115 USA.
Center for Health Decision Science, Harvard T. H. Chan School of Public Health, 718 Huntington Avenue, Boston MA 02115, USA.
Health Policy Plan. 2021 May 17;36(4):454-463. doi: 10.1093/heapol/czab026.
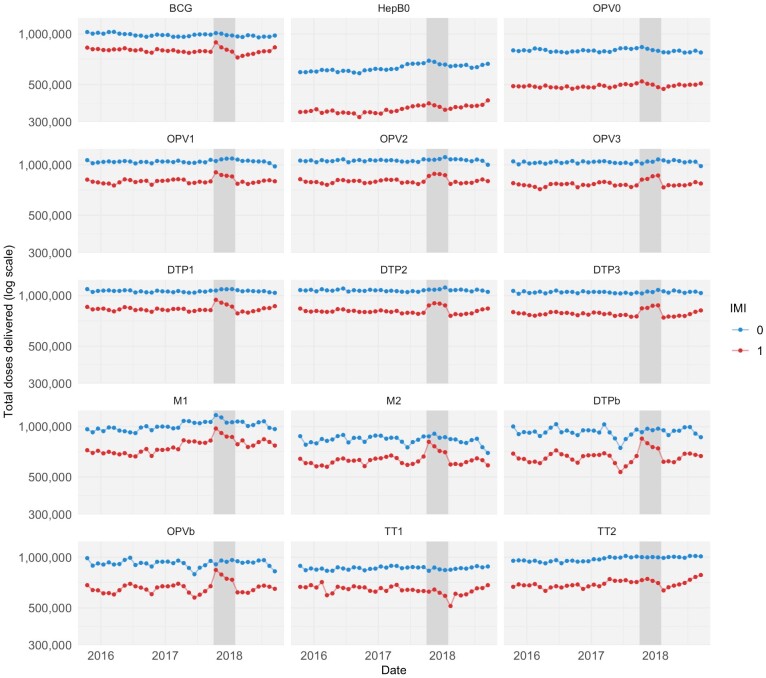
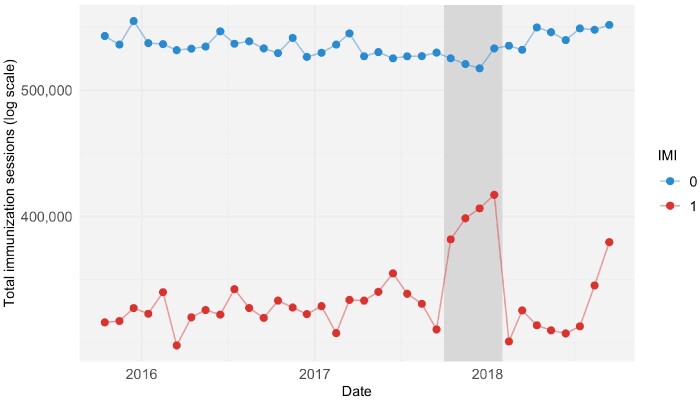
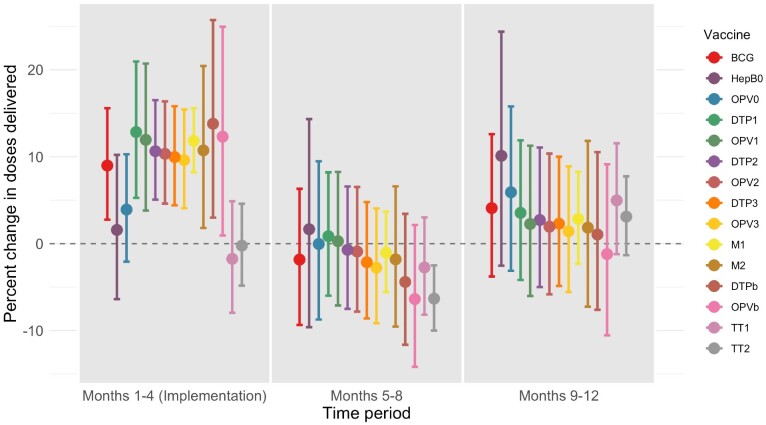
The world is not on track to achieve the goals for immunization coverage and equity described by the World Health Organization's Global Vaccine Action Plan. Many countries struggle to increase coverage of routine vaccination, and there is little evidence about how to do so effectively. In India in 2016, only 62% of children had received a full course of basic vaccines. In response, in 2017-18 the government implemented Intensified Mission Indradhanush (IMI), a nationwide effort to improve coverage and equity using a campaign-style strategy. Campaign-style approaches to routine vaccine delivery like IMI, sometimes called 'periodic intensification of routine immunization' (PIRI), are widely used, but there is little robust evidence on their effectiveness. We conducted a quasi-experimental evaluation of IMI using routine data on vaccine doses delivered, comparing districts participating and not participating in IMI. Our sample included all districts that could be merged with India's 2016 Demographic and Health Surveys data and had available data for the full study period. We used controlled interrupted time-series analysis to estimate the impact of IMI during the 4-month implementation period and in subsequent months. This method assumes that, if IMI had not occurred, vaccination trends would have changed in the same way in the participating and not participating districts. We found that, during implementation, IMI increased delivery of 13 infant vaccines, with a median effect of 10.6% (95% confidence interval 5.1% to 16.5%). We did not find evidence of a sustained effect during the 8 months after implementation ended. Over the 12 months from the beginning of implementation, we estimated reductions in the number of under-immunized children that were large but not statistically significant, ranging from 3.9% (-6.9% to 13.7%) to 35.7% (-7.5% to 77.4%) for different vaccines. The largest effects were for the first doses of vaccines against diphtheria-tetanus-pertussis and polio: IMI reached approximately one-third of children who would otherwise not have received these vaccines. This suggests that PIRI can be successful in increasing routine immunization coverage, particularly for early infant vaccines, but other approaches may be needed for sustained coverage improvements.
世界并未走上实现世界卫生组织《全球疫苗行动计划》所描述的免疫接种覆盖率和公平性目标的正轨。许多国家在努力提高常规疫苗接种的覆盖率,而且几乎没有关于如何有效做到这一点的证据。2016年在印度,只有62%的儿童接种了完整疗程的基础疫苗。作为应对措施,2017 - 18年政府实施了“强化免疫行动”(IMI),这是一项利用运动式策略提高覆盖率和公平性的全国性行动。像IMI这样的常规疫苗接种运动式方法,有时被称为“常规免疫的定期强化”(PIRI),被广泛使用,但关于其有效性的有力证据很少。我们利用已接种疫苗剂量的常规数据,对参与和未参与IMI的地区进行比较,对IMI进行了准实验评估。我们的样本包括所有能够与印度2016年人口与健康调查数据合并且在整个研究期间都有可用数据的地区。我们使用了对照中断时间序列分析来估计IMI在4个月实施期及后续月份的影响。这种方法假定,如果没有发生IMI,参与和未参与的地区的疫苗接种趋势会以相同方式变化。我们发现,在实施期间,IMI增加了13种婴儿疫苗的接种量,中位数效应为10.6%(95%置信区间为5.1%至16.5%)。我们没有发现实施结束后8个月内有持续效果的证据。在从实施开始的12个月里,我们估计不同疫苗未充分免疫儿童数量的减少幅度很大,但无统计学意义,范围从3.9%(-6.9%至13.7%)到35.7%(-7.5%至77.4%)。最大的效果是针对白喉 - 破伤风 - 百日咳和脊髓灰质炎疫苗的首剂接种:IMI覆盖了约三分之一原本不会接种这些疫苗的儿童。这表明PIRI在提高常规免疫覆盖率方面可能是成功的,特别是对于早期婴儿疫苗,但可能需要其他方法来持续提高覆盖率。