Zazzara Maria Beatrice, Palmer Katie, Vetrano Davide Liborio, Carfì Angelo, Onder Graziano
Department of Gerontology, Fondazione Policlinico Gemelli IRCCS, Rome, Italy.
Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden.
Eur Geriatr Med. 2021 Jun;12(3):463-473. doi: 10.1007/s41999-021-00481-9. Epub 2021 Mar 18.
Adverse drug reactions (ADRs) represent a common and potentially preventable cause of unplanned hospitalization, increasing morbidity, mortality, and healthcare costs. We aimed to review the classification and occurrence of ADRs in the older population, discuss the role of age as a risk factor, and identify interventions to prevent ADRs.
We performed a narrative scoping review of the literature to assess classification, occurrence, factors affecting ADRs, and possible strategies to identify and prevent ADRs.
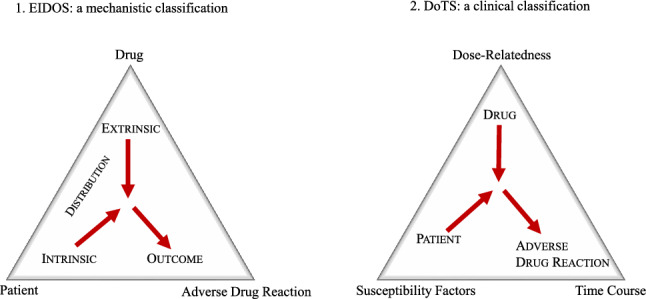
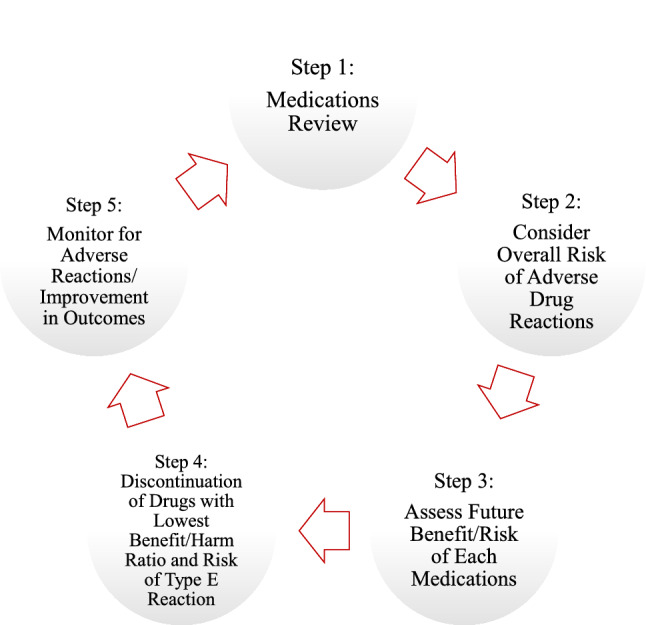
Adverse drug reactions (ADRs) are often classified as Type A and Type B reactions, based on dose and effect of the drugs and fatality of the reaction. More recently, other approaches have been proposed (i.e. Dose, Time and Susceptibility (DoTS) and EIDOS classifications). The frequency of ADRs varies depending on definitions, characteristics of the studied population, and settings. Their occurrence is often ascribed to commonly used drugs, including anticoagulants, antiplatelet agents, digoxin, insulin, and non-steroidal anti-inflammatory drugs. Age-related factors-changes in pharmacokinetics, multimorbidity, polypharmacy, and frailty-have been related to ADRs. Different approaches (i.e. medication review, software identifying potentially inappropriate prescription and drug interactions) have been suggested to prevent ADRs and proven to improve the quality of prescribing. However, consistent evidence on their effectiveness is still lacking. Few studies suggest that a comprehensive geriatric assessment, aimed at identifying individual risk factors, patients' needs, treatment priorities, and strategies for therapy optimization, is key for reducing ADRs.
Adverse drug reactions (ADRs) are a relevant health burden. The medical complexity that characterizes older patients requires a holistic approach to reduce the burden of ADRs in this population.
药物不良反应(ADR)是导致非计划住院的常见且可能可预防的原因,会增加发病率、死亡率和医疗成本。我们旨在综述老年人群中ADR的分类和发生情况,讨论年龄作为风险因素的作用,并确定预防ADR的干预措施。
我们对文献进行了叙述性范围综述,以评估ADR的分类、发生情况、影响ADR的因素以及识别和预防ADR的可能策略。
根据药物的剂量和效应以及反应的致死性,药物不良反应(ADR)通常分为A型和B型反应。最近,还提出了其他方法(即剂量、时间和易感性(DoTS)分类以及EIDOS分类)。ADR的发生率因定义、研究人群的特征和环境而异。其发生通常归因于常用药物,包括抗凝剂、抗血小板药物、地高辛、胰岛素和非甾体抗炎药。与年龄相关的因素——药代动力学变化、多种疾病、多种药物治疗和虚弱——与ADR有关。已提出不同的方法(即药物审查、识别潜在不适当处方和药物相互作用的软件)来预防ADR,并已证明可提高处方质量。然而,关于其有效性的一致证据仍然缺乏。很少有研究表明,旨在识别个体风险因素、患者需求、治疗优先级和治疗优化策略的全面老年评估是减少ADR的关键。
药物不良反应(ADR)是一个相关的健康负担。老年患者的医疗复杂性需要一种整体方法来减轻该人群中ADR的负担。