Thakkar Chirag, Joshipira Vismit
ADROIT Centre for Digestive and Obesity Surgery, Ahmedabad, Gujarat, India.
ADROIT Centre for Digestive and Obesity Surgery, Ahmedabad, Gujarat, India.
Int J Surg Case Rep. 2021 Mar;80:105634. doi: 10.1016/j.ijscr.2021.02.020. Epub 2021 Feb 16.
The incidence of Esophageal strictures following esophagitis in human immunodeficiency virus (HIV)-infected patients is profound in majority of cases. Although endoscopic dilatation remains the first line of treatment, surgery is needed for non-dilatable strictures. Sparse literature is available on clinical management for surgical intervention.
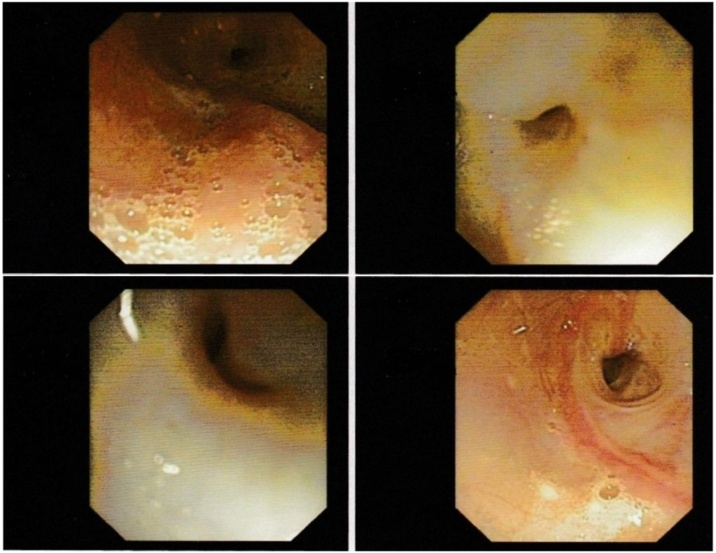
A 30 years old HIV positive male, taking ART for 10 years, presented with grade V dysphagia over long standing non-specific ulcerative esophagitis. Upper GI endoscopy revealed a long stricture starting 18 cm from the incisors. The patient underwent multiple endoscopic dilatation along with twice endoscopic stent placements over period of 2 years. As CD4 count was low associated with poor nutritional status a feeding jejunostomy was constructed. With improvement in CD4 count and nutritional status within 3 months; thoracoscopic esophagectomy, laparotomy and formation of gastric conduit and cervical anastomosis was performed. There were no intraoperative or postoperative adverse events with complete improvement in dysphagia. During follow up, 24 months after surgery the patient was on full oral diet with a total weight gain of 15 kg.
Long term solution to dysphagia due to long esophageal stricture merits a surgery in form of a replacement conduit by either stomach tube or a segment of colon. Experience and literature guiding surgical decision making are limited. Retaining or excision of the native oesophagus is still a matter of discussion.
Thoracoscopic esophagectomy with gastric tube conduit for reconstruction is a feasible and safe surgical option for esophageal stricture in a HIV infected patient.
在大多数人类免疫缺陷病毒(HIV)感染患者中,食管炎后食管狭窄的发生率很高。尽管内镜扩张仍然是一线治疗方法,但对于不可扩张的狭窄则需要手术治疗。关于手术干预的临床管理的文献很少。
一名30岁的HIV阳性男性,接受抗逆转录病毒治疗10年,因长期存在的非特异性溃疡性食管炎出现V级吞咽困难。上消化道内镜检查显示,从门牙起18厘米处有一个长狭窄。在2年的时间里,患者接受了多次内镜扩张以及两次内镜支架置入。由于CD4细胞计数低且营养状况差,进行了空肠造口术。3个月内CD4细胞计数和营养状况有所改善;随后进行了胸腔镜食管切除术、剖腹术、胃管道形成和颈部吻合术。术中及术后均无不良事件,吞咽困难完全改善。随访期间,术后24个月,患者完全经口饮食,体重增加了15千克。
对于因长段食管狭窄导致的吞咽困难,长期解决方案是采用胃管或一段结肠进行替代管道的手术。指导手术决策的经验和文献有限。保留或切除原生食管仍是一个有争议的问题。
胸腔镜食管切除术加胃管重建术是治疗HIV感染患者食管狭窄的一种可行且安全的手术选择。