Division of Biostatistics, Department of Public Health Sciences, Medical University of South Carolina, Charleston, South Carolina, United States of America.
Charleston Health Equity and Rural Outreach Innovation Center (HEROIC), Ralph H. Johnson VA Medical Center, Charleston, South Carolina, United States of America.
PLoS One. 2021 Mar 24;16(3):e0248702. doi: 10.1371/journal.pone.0248702. eCollection 2021.
Socially vulnerable communities may be at higher risk for COVID-19 outbreaks in the US. However, no prior studies examined temporal trends and differential effects of social vulnerability on COVID-19 incidence and death rates. Therefore, we examined temporal trends among counties with high and low social vulnerability to quantify disparities in trends over time.
We conducted a longitudinal analysis examining COVID-19 incidence and death rates from March 15 to December 31, 2020, for each US county using data from USAFacts. We classified counties using the Social Vulnerability Index (SVI), a percentile-based measure from the Centers for Disease Control and Prevention, with higher values indicating more vulnerability. Using a Bayesian hierarchical negative binomial model, we estimated daily risk ratios (RRs) comparing counties in the first (lower) and fourth (upper) SVI quartiles, adjusting for rurality, percentage in poor or fair health, percentage female, percentage of smokers, county average daily fine particulate matter (PM2.5), percentage of primary care physicians per 100,000 residents, daily temperature and precipitation, and proportion tested for COVID-19.
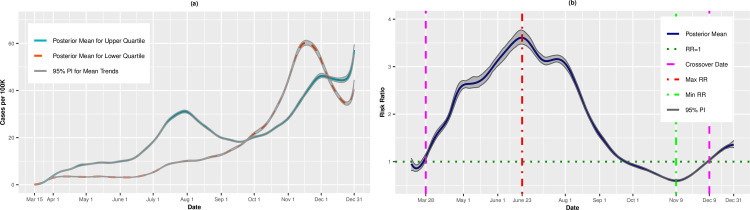
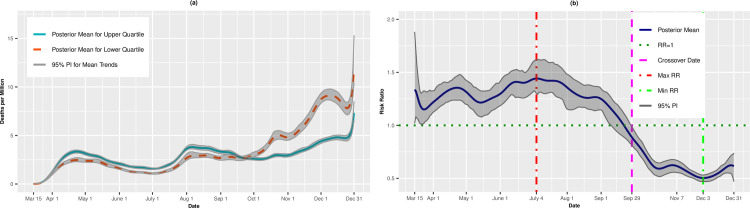
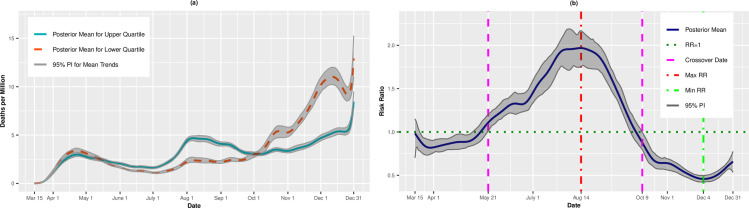
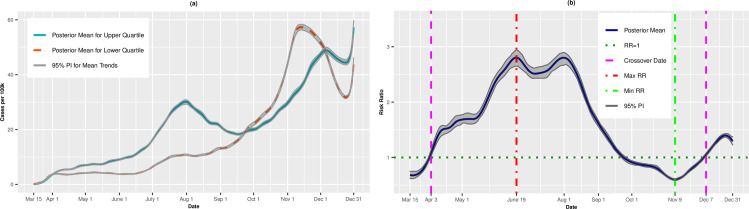
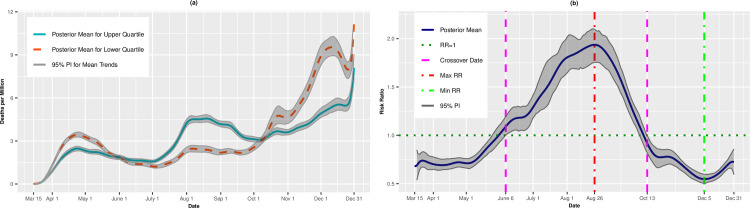
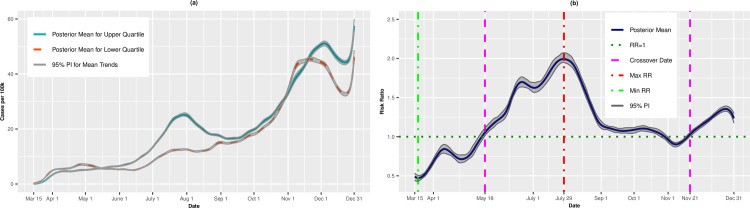
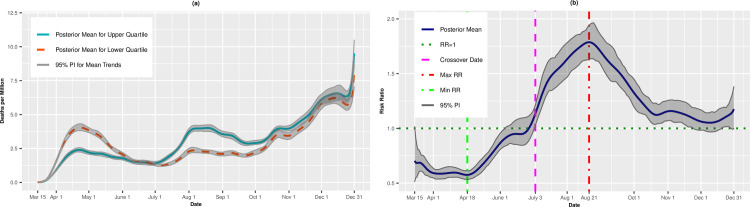
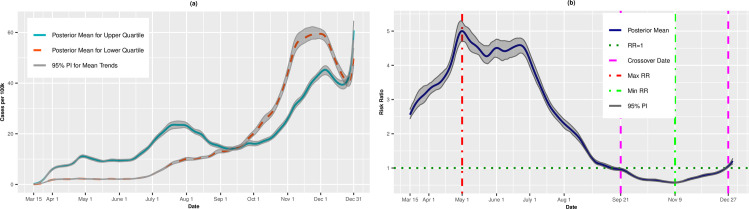
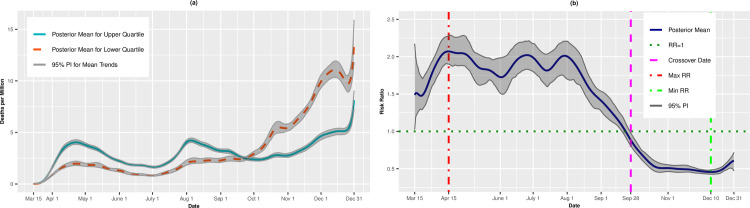
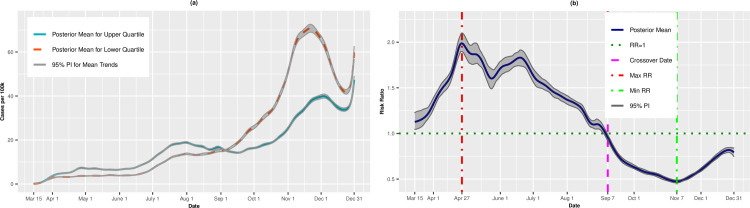
At the outset of the pandemic, the most vulnerable counties had, on average, fewer cases per 100,000 than least vulnerable SVI quartile. However, on March 28, we observed a crossover effect in which the most vulnerable counties experienced higher COVID-19 incidence rates compared to the least vulnerable counties (RR = 1.05, 95% PI: 0.98, 1.12). Vulnerable counties had higher death rates starting on May 21 (RR = 1.08, 95% PI: 1.00,1.16). However, by October, this trend reversed and the most vulnerable counties had lower death rates compared to least vulnerable counties.
The impact of COVID-19 is not static but can migrate from less vulnerable counties to more vulnerable counties and back again over time.
在美国,社会弱势群体社区可能面临更高的 COVID-19 爆发风险。然而,之前没有研究考察社会脆弱性对 COVID-19 发病率和死亡率的时间趋势和差异影响。因此,我们研究了社会脆弱性程度较高和较低的县的时间趋势,以量化随着时间的推移趋势的差异。
我们使用来自 USAFacts 的数据,对 2020 年 3 月 15 日至 12 月 31 日期间每个美国县的 COVID-19 发病率和死亡率进行了一项纵向分析。我们使用疾病控制与预防中心的社会脆弱性指数(SVI)对县进行分类,该指数是基于百分位数的衡量标准,数值越高表示脆弱性越高。使用贝叶斯分层负二项模型,我们估计了比较 SVI 第一(较低)和第四(较高)四分位数的县的每日风险比(RR),调整了农村、健康状况不佳或中等的百分比、女性百分比、吸烟者百分比、县平均每日细颗粒物(PM2.5)、每 10 万居民的初级保健医生比例、每日温度和降水以及 COVID-19 检测比例。
在大流行开始时,最脆弱的县每 10 万人口的病例数平均少于最不脆弱的 SVI 四分位数。然而,在 3 月 28 日,我们观察到一个交叉效应,即最脆弱的县的 COVID-19 发病率高于最不脆弱的县(RR = 1.05,95%PI:0.98,1.12)。从 5 月 21 日开始,脆弱县的死亡率更高(RR = 1.08,95%PI:1.00,1.16)。然而,到 10 月,这种趋势发生了逆转,最脆弱的县的死亡率低于最不脆弱的县。
COVID-19 的影响不是静态的,而是随着时间的推移可以从脆弱性较低的县转移到脆弱性较高的县,然后再返回。