Department of Cardiology, Croydon Health Service, London, UK.
School of Biomedical Engineering and Imaging Sciences, Kings College London, London, UK.
Heart Fail Rev. 2022 Jan;27(1):251-261. doi: 10.1007/s10741-021-10087-9. Epub 2021 Mar 24.
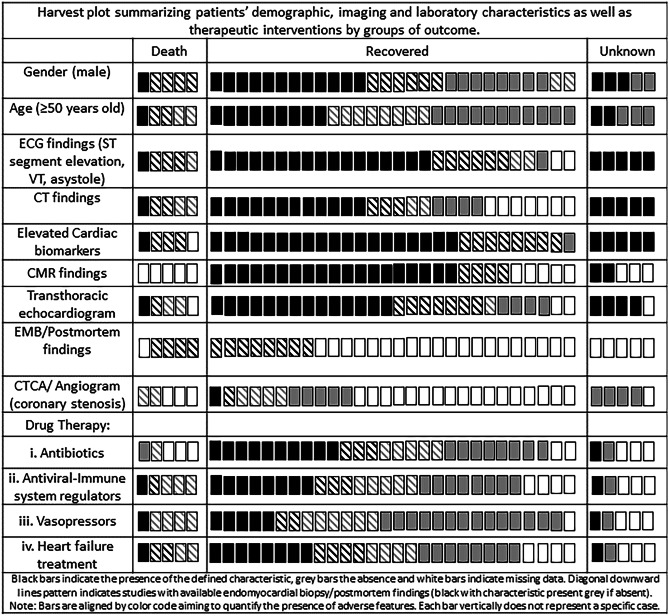
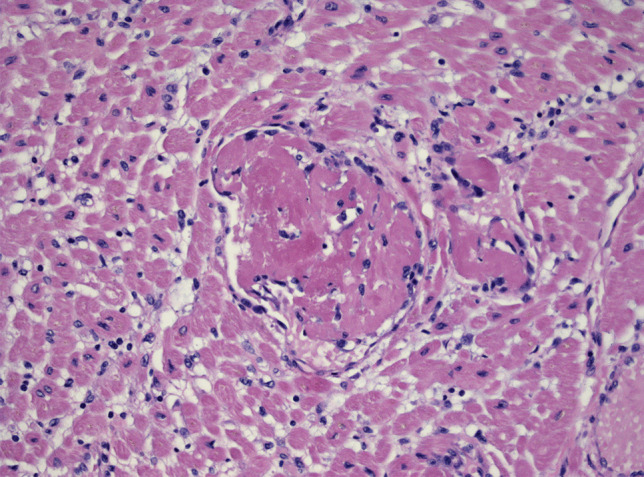
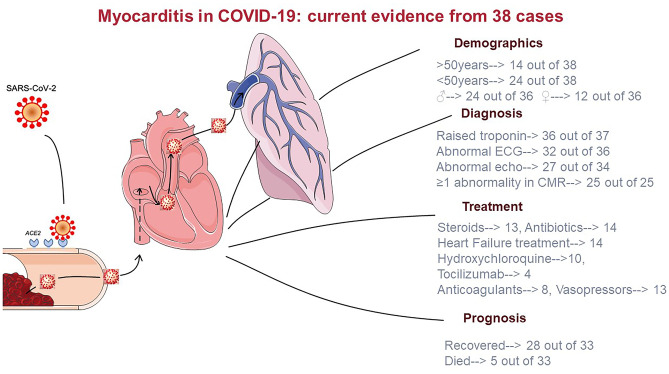
Myocardial inflammation in COVID-19 has been documented. Its pathogenesis is not fully elucidated, but the two main theories foresee a direct role of ACE2 receptor and a hyperimmune response, which may also lead to isolated presentation of COVID-19-mediated myocarditis. The frequency and prognostic impact of COVID-19-mediated myocarditis is unknown. This review aims to summarise current evidence on this topic. We performed a systematic review of MEDLINE and Cochrane Library (1/12/19-30/09/20). We also searched clinicaltrials.gov for unpublished studies testing therapies with potential implication for COVID-19-mediated cardiovascular complication. Eligible studies had laboratory confirmed COVID-19 and a clinical and/or histological diagnosis of myocarditis by ESC or WHO/ISFC criteria. Reports of 38 cases were included (26 male patients, 24 aged < 50 years). The first histologically proven case was a virus-negative lymphocytic myocarditis; however, biopsy evidence of myocarditis secondary to SARS-CoV-2 cardiotropism has been recently demonstrated. Histological data was found in 12 cases (8 EMB and 4 autopsies) and CMR was the main imaging modality to confirm a diagnosis of myocarditis (25 patients). There was a substantial variability in biventricular systolic function during the acute episode and in therapeutic regimen used. Five patients died in hospital. Cause-effect relationship between SARS-CoV-2 infection and myocarditis is difficult to demonstrate. However, current evidence demonstrates myocardial inflammation with or without direct cardiomyocyte damage, suggesting different pathophysiology mechanisms responsible of COVID-mediated myocarditis. Established clinical approaches should be pursued until future evidence support different actions. Large multicentre registries are advisable to elucidate further.
COVID-19 患者存在心肌炎症。其发病机制尚未完全阐明,但两种主要理论预测 ACE2 受体的直接作用和过度免疫反应,这也可能导致 COVID-19 介导的心肌炎孤立表现。COVID-19 介导的心肌炎的频率和预后影响尚不清楚。本综述旨在总结该主题的现有证据。我们对 MEDLINE 和 Cochrane 图书馆(12 月 1 日至 9 月 30 日)进行了系统综述。我们还在 clinicaltrials.gov 上搜索了正在测试对 COVID-19 介导的心血管并发症具有潜在影响的治疗方法的未发表研究。符合条件的研究具有实验室确诊的 COVID-19 ,并根据 ESC 或 WHO/ISFC 标准进行了临床和/或组织学诊断的心肌炎。报告了 38 例病例(26 名男性患者,24 名年龄<50 岁)。首例经组织学证实的病例为病毒阴性淋巴细胞性心肌炎;然而,最近已经证明了 SARS-CoV-2 心脏嗜性引起的心肌炎的活检证据。在 12 例(8 例 EMB 和 4 例尸检)中发现了组织学数据,并且 CMR 是确认心肌炎诊断的主要成像方式(25 例)。在急性发作期间和治疗方案中,左右心室收缩功能存在很大差异。5 例患者在医院死亡。很难证明 SARS-CoV-2 感染与心肌炎之间的因果关系。然而,目前的证据表明存在心肌炎症,伴有或不伴有直接心肌细胞损伤,提示 COVID 介导的心肌炎有不同的病理生理机制。应采用既定的临床方法,直至获得支持不同治疗措施的进一步证据。建议进行大型多中心登记研究以进一步阐明。